Intensive Insulin Therapy in Surgical Patients with Type 2 Diabetes Mellitus
The aim of the investigation was to assess the efficiency of intensive insulin therapy in surgical patients with type 2 diabetes mellitus (DM 2) in intensive care unit in relation to the effect on postoperative clinical progression and 90-day survival of patients.
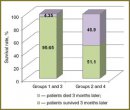
Materials and Methods. The study included 89 patients hospitalized in intensive care unit for various surgical pathologies, with DM 2 in past medical history. On admission the patients were divided into 4 groups in a random manner. First 72 h target glycemia range for groups 1 and 2 was glucose level of 6.5–8.5 mmol/L, and for groups 3 and 4 — 8.6–11.0 mmol/L. Continuous insulin infusion was chosen for the treatment of groups 1 and 3 for the same period, the patients of groups 2 and 4 were given divided insulin injections. The severity of all patients was studied first 24 h and 72 h after inpatient treatment according to APACHE II, SAPS II.
Conclusion. In ICU patients suffering from type 2 DM with various surgical pathology, target glycemic levels of 6.5–8.5 and 8.6–11.0 within the frame of one insulin therapy method are not associated with the differences in relation to the severity and outcome of the main pathology. Glycemic control in target range of 6.5–11.0 mmol/L by intravenous insulin infusion has the advantage over divided insulin subcutaneous injections regarding the severity and outcome of the main pathology.
- Galstyan G.R. Khronicheskie oslozhneniya sakharnogo diabeta: etiopatogenez, klinika, lechenie [Chronic complication of diabetes mellitus: etiopathogenesis, clinical picture, theatment]. Rus Med Z — Russian Medical Journal 2004; 23(12): 51–54.
- Branco R.G., Tasker R.C., Garcia P.C., Piva J.P., Xavier L.D. Glycemic control and insulin therapy in sepsis and critical illness. J Pediatr (Rio J) 2007; 83: 128–136.
- McAlister F.A., Majumdar S.R., Blitz S., et al. The relation between hyperglycemia and outcome in 2,471 patients admitted to the hospital with community-acquired pneumonia. Diabetes Care 2005; 28(4): 810–815.
- Van den Berghe G., Wilmer A., Hermans G., et al. Intensive insulin therapy in the medical ICU. N Engl J Med 2006; 354: 449–461.
- Brunkhorst F.M., Engel C., Bloos F., et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med 2008; 358(2): 125–139.
- Devos P., Preiser J., Melot C. Impact of tight glucose control by intensive insulin therapy on ICU mortality and the rate of hypoglycemia: final results of the glucontrol study. Intensive Care Med 2007; 33(Suppl 2): S189.
- He W., Zhang T.Y., Zhou H., Li T., Zhao J.Y., Zhao D., Liu X.H., Hou J., Wang C., Xu Y. Impact of intensive insulin therapy on surgical critically ill patients. Zhonghua Wai Ke Za Zhi 2007 Aug; 45(15): 1052–1054.
- Dellinger R.P., Levy M., Carlet J., et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Med 2008; 34(1): 17–60.
- Michigan Health and Safety Coalition. A toolkit for intensive care units to improve the safety and quality of patient care. http: //www.mihealthandsafety.org/icu/9.htm. 2008.
- Rodbard H.W., Blonde L., Braithwaite S.S., Brett E.M., Cobin R.H., Handelsman Y., et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the management of diabetes mellitus. Endocr Pract 2007; 13(Suppl 1): 1–68.
- American Diabetes Association. Standards of medical care in diabetes — 2008. Diabetes Care 2008; 31(Suppl 1): S12–S54.
- Mackenzie I., Ingle S., Zaidi S., Buczaski S. Tight glycaemic control: a survey of intensive care practice in large English hospitals. Intensive Care Med 2005; 31(8): 1136.
- Finfer S., Chittock D.R., Su S.Y., Blair D., Foster D., Dhingra V., et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med Mar 2009; 360(13): 1283–1297.
- Kutcher M.E., Pepper M.B., Morabito D., Sunjaya D., Knudson M.M., Cohen M.J. Finding the sweet spot: identification of optimal glucose levels in critically injured patients. J Trauma 2011 Nov; 71(5): 1108–1114.
- Griesdale D.E., de Souza R.J., van Dam R.M., et al. Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE-SUGAR study data. CMAJ 2009; 180: 821–827.
- Wiener R.S., Wiener D.C., Larson R.J. Benefits and risks of tight glucose control in critically ill adults: a meta-analysis. JAMA 2008; 300(8): 933–944.
- McMullin J., Brozek J., Jaeschke R., et al. Glycemic control in the ICU: a multicenter survey. Intensive Care Med 2004; 30(5): 798–803.
- Clement S., Braithwaite S.S., Magee M.F., et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care 2004. 27: 553–591.
- Garber A.J., Moghissi E.S., Bransome E.D.Jr., et al. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocrinol Pract 2004; 10:77–82.
- Algoritmy spetsializirovannoy meditsinskoy pomoshchi bol’nym sakharnym diabetom [Schemes of specialized medical care for diabetics]. Pod red. Dedova I.I., Shestakovoy M.V. [Dedov I.I., Shestakova M.V. (editors)] Moscow; 2011.
- Marik P.E., Preiser J.C. Toward understanding tight glycemic control in the ICU: a systematic review and metaanalysis. Chest 2010 Mar; 137(3): 544–551.








