Diagnostic Value Sonoelastography in Differential Diagnosis of Thyroid Nodules
The aim of the investigation was to assess the reliability of main sonoelastographic diagnostic criteria of thyroid cancer and determine sonoelastography efficiency in pre-operative diagnostics of thyroid nodules based on a complex of radiological, cytologic and histologic methods.
Materials and Methods. The study involved 372 patients with thyroid nodules, among them there were 87 (13%) male and 285 (87%) female patients; mean age being 44.90±0.30 years. All the patients underwent standard diagnostic procedures: an endocrinal examination, a hormone laboratory test, an ultrasound investigation using color flow Doppler supplemented by sonoelastography, as well as fine-needle aspiration biopsy of nodules followed by cytologic analysis.
Results. Diagnosis of “adenoma or cancer” in 80 patients (95%) made on the basis of sonoelastographic and cytologic findings was confirmed by histologic examination of surgical materials. Sonoelastography sensitivity in thyroid cancer detection is 95.3%, specificity — 98.2%, diagnostic accuracy — 96%.
Conclusion. Qualitative elastographic characteristics of nodules (blue staining) and quantitative value of strain ratio, which equals to over 4, are high-specific in pre-operative thyroid cancer diagnosis. Sonoelastography application improves the diagnostic accuracy of a pre-operative diagnostic complex of thyroid nodule facilitating the management of patients with thyroid pathology.
Development and implementation of new and more effective diagnostic methods for revealing early forms of malignant neoplasms of thyroid gland allow surgeons to choose the most adequate extension of the operation and obtain good remote treatment results at the preoperative stage [1, 2]. One of such techniques along with a fine-needle aspiration biopsy is sonoelastography (SEG). SEG is a method of visualization, based on the difference of elastic properties of the tissues. Unequal degree of deformation of various organ tissues under a slight compression, determined by an ultrasound device, forms the bases for this method [3]. However, in the current literature there are not enough data on the informativity of this technique, and correlation of SEG values with the data of preoperative (cytological) and post-operative (histological) investigations of thyroid cancer patients is not studied either [4, 5].
The aim of investigation is to assess reliability of the main sonoelastographic diagnostic criteria of thyroid cancer according to the data of comparing the values of the complex of radiological, cytological and histological methods, and to determine the role and efficacy of sonoelastography in preoperative diagnosis of nodule formation of the thyroid gland.
Materials and Methods. The study involved 372 patients with nodular thyroid gland, among them there were 87 (13%) males and 285 (87%) females, mean age being 44.90±0.30 years. All patients underwent a standard complex of diagnostic procedures: examination by endocrinologist, laboratory investigations of hormone status, ultrasound examination with color Doppler mapping, supplemented by SEG, as well as fine-needle aspiration biopsy of the nodules followed by cytological studies. On the basis of the conducted diagnostic procedures nodular colloid goiter was diagnosed in 201 cases (54%), toxic goiter in 52 (14%) cases, autoimmune thyroiditis in 35 (9.4%) cases, thyroid adenoma in 31(8.3%), thyroid cancer in 53 (14.3%). Surgical treatment with the following histological investigation of the operation material was administered to 84 patients.
Sonoelastographic investigation with obtaining images was performed using HITACHI EUB HI VISION 900 scanner (Japan) with a linear high frequency transducer having 8–12 Hz frequency and moderate transducer pressure. During SEG the assessment of nodule rigidity coefficient was made. Elastograms were evaluated according to computerized color scale, where the degree of rigidity corresponded to a definite color, and also according to a standard score rigidity scale. Staining of the nodule during SEG in blue colors and coefficient of deformation (CD) more than 4 were considered to be the signs of malignant tumors, staining in red-green colors and CD less than 3 — the signs of benign ones. Coefficient of deformation was counted by the device automatically using comparative analysis of the elasticity of the node and that of the adjoining relatively intact tissue.
Punctates of the thyroid gland, obtained by aspiration puncture with a fine needle under ultrasound examination control, and intraoperational scrapings from the tumor tissue served the material for cytological examination. The material was stained by azure-eosine solution according to May-Gürnvald [6].
Preparations were investigated under a light microscope. Methodological principles of investigation involved obligatory examination of the specimen margines along the whole perimeter and double cross analysis of multiple fields of view. The findings of the cytological examination were considered to be acceptable only if it was conducted on the adequate material following all methodological requirements [7, 8].
An operational material was delivered to the Anatomic Pathology Department of City Hospital No.33 (Nizhny Novgorod), where its macro- and microscopic study was carried on. Sampling of fragments for examination was made from thyroid nodules with detailed description of their character and dimensions. The material was fixed in 10% formalin at 37°C for 24 h, and then dehydrated. After placement in xylene, it was imbedded in paraffin. Then, sections 5 μm thick were stained with hematoxylin-eosine. For morphometric processing and creation of videoarchive of the material obtained microscope Nikon 1001 (Germany) with X90, X40, X15 lenses was used. Computer analysis of cytological and histological specimens was conducted using a system of image analysis, consisting of a light transmission microscope ECLIPS (Nikon, Germany), computer Pentium IV IBM, color digital videocamera DS, control unit DS-U1 (Nikon, Germany), and software ФCT-2U.
The study complied with the Declaration of Helsinki (The Declaration was passed in Helsinki, Finland in June, 1964 and revised in October, 2000 (Edinburg, Scotland) and was performed following approval by the Ethic Committee of Nizhny Novgorod Regional Medical Association. Written informed consent was obtained from every patient for conducting minimally invasive investigations and operative intervention.
Results and Discussion. According to the data of the conducted investigation, 288 patients (77.7%) with diagnosis of “nodular colloid goiter, nodular toxic goiter, autoimmune thyroiditis” were left for dynamic follow-up. Surgery was performed on 84 patients (22.6%) with preoperative diagnosis “adenoma or cancer”, made on the basis of cytological examination and SEG. Findings of preoperative diagnosis were compared to the materials of histological study of the surgical specimens.
According to the results of SEG benign adenomatous changes looked like foci of mosaic structure, in which zones of increased and reduced density with CD≤3 were observed. On the basis of cytological examination findings a conclusion of follicular tumor was made. Malignant neoplasms in SEG were stained homogeneously in blue colors, in separate cases blue areas overrun the borders of the focus, which spoke of infiltrative tumor growth. CD>4. Cytological investigations stated papillary cancer, or follicular tumor.
After histological examination of the operation material, the diagnosis of “adenoma of thyroid gland” was made to 29 patients (36.9%). In all cases a single nodule with a clear capsule was determined. Nodules were homogeneous in their structure. Morphological study divided adenomas into microfollicular — 18 cases (60%), which represented areas of parenchimatous structure with formation of tiny follicles, and trabecular — 11 cases (40%), representing during histological study multiple bands of epithelial cells, forming trabecular structures.
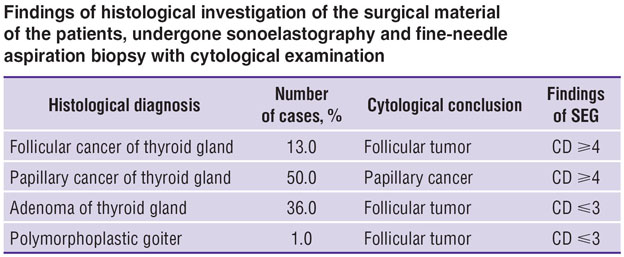
The diagnosis “thyroid cancer”, based on histological examination, was made to 51 patients (63%). Of them papillary cancer was revealed in 42 cases (81%), microscopically these tumors were seen as nodules of dense consistency, whitish or light-brown color. Commonly, such nodules had thin fibrous or rough capsule made of fibrous tissue. In a number of cases tumors were determined to have no distinct borders with the surrounding tissues. Sizes varied from 0.5 to 6.5 cm. Morphological examination showed tumors to have characteristic papilla formation, which spread out both in cystic cavities and in the gland itself. Follicular cancer, found in 9 patients (19%), under macroscopic study of the surgical material was presented more often by single nodules from 1.5 to 5 cm in diameter. All nodules had a fibrous capsule. The diagnosis of “follicular cancer” was made on the basis of revealing follicular or follicular-solid structures and absence of papillas [9]. Four patients (1%) were made a diagnosis of “nodular colloid polimorphoplastic goiter” according to the findings of histological investigation (See the Table).
|
Findings of histological investigation of the surgical material of the patients, undergone sonoelastography and fine needle aspiration biopsy with cytological examination |
Comparison of the SEG and cytological data showed, that the diagnosis was confirmed in 80 patients (95%) by the findings of histological investigation of the material, taken during operative intervention. Sensitivity of SEG for revealing thyroid cancer amounted to 95.3%, specificity — 98.2%, diagnostic accuracy — 96%. The data obtained by us demonstrate, that sonoelastography technique cannot become an alternative to the morphological study, but its application increase the diagnostic significance of preoperative diagnosis of the nodular pathology of thyroid gland. Using criteria of ultrasound diagnosis in SEG mode improves the quality of following up patients with nodulation of thyroid gland and helps in choosing a more precise treatment tactics for the patients with this pathology.
Conclusion. Qualitative elastographic characteristics of nodules (staining in blue colors) and quantitative value of coefficient of deformation more than 4 are highly specific for preoperative diagnosis of thyroid cancer. Sonoelastography allows to define the most important damaged area of the organ for making target puncture biopsy.
Application of sonoelastography in the dynamic follow-up of patients with a nodular pathology of thyroid gland improves the diagnostic accuracy of the preoperative diagnosis.
Study Funding and Competing Interests. The study was not supported by any financial sources, and there is no conflict of interest related to the authors.
References
- Prakticheskoe rukovodstvo po ul’trazvukovoy diagnostike. Obshchaya ul’trazvukovaya diagnostika [Practice guidelines on ultrasound diagnostics. General ultrasound diagnosis]. Pod red. Mit’kova V.V. [Mit’kov V.V. (editor)]. Moscow: Vidar; 2005; 698 p.
- Giordano D., Valcavi R., Thompson G.B., Pedroni C., Renna L., Gradoni P., Barbieri V. Complications of central neck dissection in patients with papillary thyroid carcinoma: results of a study on 1087 patients and review of the literature. Thyroid 2012; 22(9): 911–917, http://dx.doi.org/10.1089/thy.2012.0011. Epub 2012 Jul 24.
- Park C.S., Kim S.H., Jung S.L., Kang B.J., Kim J.Y., Choi J.J., Sung M.S., Yim H.W., Jeong S.H. Observer variability in the sonographic evaluation of thyroid nodules. J Clin Ultrasound 2010; 38(6): 287–293, http://dx.doi.org/10.1002/jcu.20689.
- Yu-rong Hong, Yu-lian Wu, Zhi-yan Luo, Ning-bo Wu, Xue-ming Liu. Impact of nodular size on the predictive values of gray-scole, color–Doppler ultrasound end sonoelastography for assessment of thyroid nodules. J Zhejiang Univ Sci B 2012 Sept; 13(9): 707–716, http://dx.doi.org/10.1631/jzus.B1100342.
- Khokhlova E.A., Zubarev A.V., Rozhkova N.I. Vozmozhnosti sonoelastografii v utochnyayushchey diagnostike zabolevaniy molochnykh zhelez [Sonoelastography capabilities in specifying diagnostics of breast diseases]. Kremlevskaya meditsina. Klinicheskiy vestnik — Kremlin Medicine. Clinical Vestnik 2009; 3: 41–48.
- Korzhevskiy D.E., Gilyarov A.V. Osnovy gistologicheskoy tekhniki [Basics of histological techniques]. Saint Petersburg: SpetsLit., 2010.
- Samir A.E., Vij A., Seale M.K., Desai G., Halpern E., Faquin W.C., Parangi S., Hahn P.F., Daniels G.H. Ultrasound-guided percutaneous thyroid nodule core biopsy: clinical utility in patients with prior nondiagnostic fine-needle aspirate. Thyroid 2012; 22(5): 461–467, http://dx.doi.org/10.1089/thy.2011.0061.
- The Bethesda system for reporting thyroid cytopathology. Definitions. Criteria and explanatory notes. Syed Z. Ali, Edmund S. Cibas (Eds.). Springer; 2010.
- Abrosimov A.Yu., Kazantseva I.A., Lushnikov E.F. Morfologicheskaya diagnostika zabolevaniy shchitovidnoy zhelezy [Morphological diagnosis of thyroid diseases]. Moscow: OOO «MK»; 2012.









