The Capabilities of Advanced Echography Techniques in Diagnosis of Gastric Submucous Masses
The aim of the investigation was a comparative study of the possibilities of modern ultrasound diagnostic techniques (sonoelastography and amplitude sonohistography) to reveal gastric submucous masses.
Materials and Methods. 61 patients with gastric submucous masses were examined. All patients underwent esophagogastroduodenoscopy and ultrasound on apparatuses Aplio MX (Toshiba, Japan), Hitachi HI VISION Preirus (Japan), Voluson 730 Expert (GE, USA) with 3.5–12 MHz sensors, using sonoelastography and amplitude sonohistography. 12 patients underwent endoscopic ultrasound investigation. The diagnoses were morphologically verified (bioptates, operative material). Sonoelastography was used to determine a mass strain ratio — SR (Strain Ratio). Amplitude sonohistography to determine histographic index (I) was used as an additional method to determine density and elasticity of tumors.
Results. Qualitative parameters of sonographic signs of gastric submucous masses do not always enable to determine the presence of malignant transformation. The most challenging in differential diagnosis are gastric submucous infiltrates either of ulcerative or cancer origin, lymphomas, and aberrant (ectopic) pancreas. Resistance index (RI) of arterial vessels of the tumors, histographic index, and strain ratio appeared to be the most informative ones among quantitative parameters of sonographic signs of gastric submucous masses. There is a clear tendency for histographic index decrease and SR increase in gastric malignant submucous tumors.
Conclusion. Complex ultrasound diagnosis using advanced techniques and technologies (sonoelastography and amplitude sonohistology) is a sensitive and precise method to reveal gastric submucous tumors. Joint use of ultrasound and endoscopy promotes more qualitative use of differential diagnosis and making adequate management.
Gastric submucous masses amount to 0.5–5% among all upper gastrointestinal tumors. Life-time diagnosis enables to reveal these tumors in 4–5% population [1]. At the same time postmortem studies of patients over 50 have shown submucous masses to be newly found in 50% cases. Diagnosis and management of these tumors in contrast to epithelial neoplasms are more difficult, and require a complex approach using modern endoscopic and radiological methods, the study of tumor histological structure, the detalization of intra- and extra-organ expansion of a neoplastic process. Tumor invasion of the organ wall is the main parameter when choosing a treatment modality. Continuous technical improvement of equipment and the emergence of new endoscopic and radiological techniques contribute to a problem solution [2, 3]. The published findings of studies using sonoelastography [4–8] have proved the efficiency of this technique in ultrasound diagnostics of neoplasms. Thus, it can be supposed that this method can be applied to study gastric submucous masses as well.
The aim of the investigation was a comparative study of the possibilities of modern ultrasound diagnostic techniques (sonoelastography and amplitude sonohistography) to reveal gastric submucous masses.
Materials and Methods. 61 patients with gastric submucous masses underwent treatment in Republican Clinical Hospital No.2, Kazan, in 2004–2013. Among them there were 38 female and 23 male patients, aged 21–78 years. All patients underwent esophagogastroduodenoscopy and ultrasound on apparatuses Aplio MX (Toshiba, Japan), Hitachi HI VISION Preirus (Japan), Voluson 730 Expert (GE, USA) with 3.5–12 MHz sensors (for better visualization the stomach was 500–600 ml water-filled). Ultrasound with sonoelastography was performed in 32 patients, amplitude sonohistography — in 38 patients, ultrasound angiography — in 54 patients; 12 patients underwent endoscopic ultrasound investigation. All diagnoses were morphologically verified (bioptates, operative material).
The study complies with the declaration of Helsinki (adopted in June, 1964 (Helsinki, Finland) and revised in October, 2000 (Edinburg, Scotland)), and was performed following approval by the ethic committee of Kazan State Medical Academy. Written informed consent was obtained from all patients.
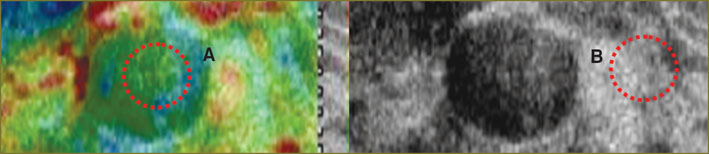
Quantitative sonoelastography was used to determine a mass strain ratio — SR (Strain Ratio) by comparative analysis of eleasticity of the mass itself (A) and the elasticity of adjacent intact tissue (B): SR=B/A (Fig. 1). Quantitative assessment of ultrasonic images of organs and tissues by amplitude sonohistograming — amplitude sonohistography (ASH) — was used as an additional method to determine tumor density and elasticity. The technique includes the marking an object area by directing a sensor to an object, the construction and analysis of sonohistograms, the calculation of a dominant gray scale step for a certain organ area. Mean value of a dominant gray scale step determined in the area under study characterizes tissue echodensity (P): Р=М/Т·L, where T — an average pixel number; M — number of pixels having L value in the area under study; L — a dominant gray scale step. Histographic index (I) of the test object is more significant: I=B/S·L, where B is histogram base width; S — a start interval; L — a dominant gray scale step (Fig. 2). For ASH we used the following conditions: constant ultrasound scanner settings (brightness, contrast, sensitivity, signal focusing and power — Gain); equal areas of comparable zones that should provide a fixed area of histographic image (Fig. 3).
|
Fig. 1. Strain ratio in sonoelastography, SR=B/A. А — tumor elasticity; В — elasticity of adjacent intact tissue |
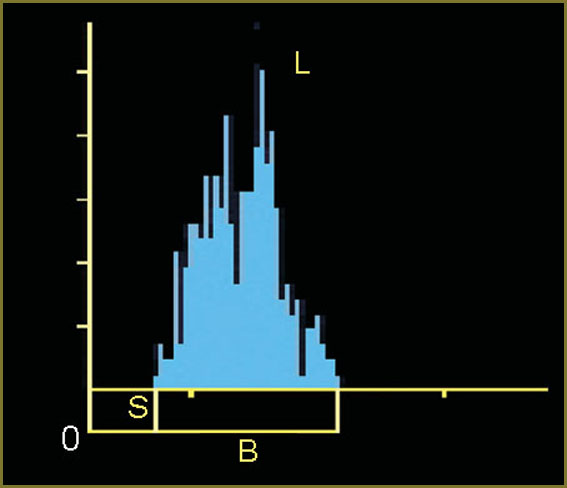 Fig. 2. Amplitude sonohistography. B — histogram base width; S — a start interval; L — a dominant gray scale step Fig. 2. Amplitude sonohistography. B — histogram base width; S — a start interval; L — a dominant gray scale step
|
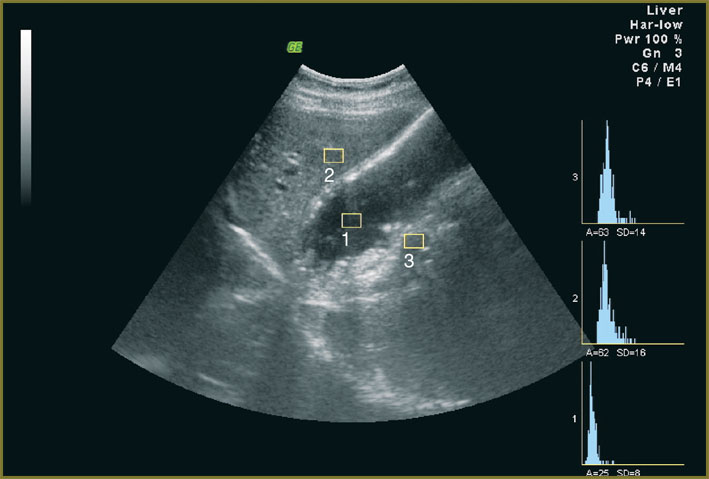 Fig. 3. Sonohistograms of gastric cavity (1), liver (2), gastric wall (3) Fig. 3. Sonohistograms of gastric cavity (1), liver (2), gastric wall (3)
|
For the sake of convenience in this study we used a modified classification of gastric submucous tumors by their frequency, the classification including also submucous ulcerative infiltrate with restored mucosa and gastric endophytic carcinoma.
Benign gastric submucous masses: 1) submucous ulcerative infiltrate; 2) lipoma; 3) fibroma; 4) fibrolipoma; 5) leiomyoma; 6) aberrant (ectopic) pancreas; 7) hamartoma; 8) schwannoma; 9) other tumors.
Malignant gastric submucous tumors: 1) submucous (endophytic) carcinoma; 2) liposarcoma; 3) fibrosarcoma; 4) leiomyosarcoma; 5) lymphoma; 6) lymphosarcoma; 7) lymphangioma; 8) others.
Results and Discussion. Ultrasound investigation was performed in patients with gastric submucous tumors to determine qualitative and quantitative parameters of ultrasonographic signs. Qualitative indices included ultrasonographic data on the outer contour (clear, blurred), echogenicity (anechoic, hypo-, iso-, hyperechoic), structure (homogeneous, heterogeneous), integrity of gastric mucosa (solution of continuity, unimpaired integrity, restored integrity), gastric peristalsis in the area of interest (dysperistalsis, normal peristalsis), type and character of tumor vascularization (avascular, hypo-, hypervascular, normal vascularization, mosaic vascularization). The following ultrasonographic data were referred to quantitative indices: gastric wall thickness in damage area (in mm), size (maximum length and width, in mm), resistance index (RI) of tumor arterial vessels, histographic index (I), strain ratio (SR).
Clinical examples
1. Patient S., aged 47, with “infiltrative ulcer of lesser curvature of stomach” (Fig. 4). Ultrasonographic signs: 1) clear contours; 2) thickening of a submucous layer up to 6–8 mm; 3) low echogenicity; 4) restored integrity of mucous layer; 5) normal peristalsis; 6) good vascularization, RI=0.59; 7) histographic index I=0.33; 8) strain ratio in sonoelastography SR=0.96.
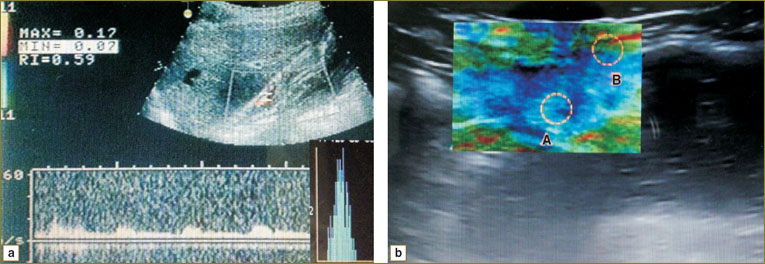 Fig. 4. Sonohistogram (а) and sonoelastogram (b) of patient S. Infiltrative ulcer of lesser curvature of stomach. А — elasticity in infiltration area, В — elasticity of healthy gastric wall Fig. 4. Sonohistogram (а) and sonoelastogram (b) of patient S. Infiltrative ulcer of lesser curvature of stomach. А — elasticity in infiltration area, В — elasticity of healthy gastric wall
|
2. Female patient К., aged 58, with gastric leiomyoma (Fig. 5). Ultrasonographic signs: 1) clear irregular contours; 2) medium echogenicity; 3) thin mucous layer above the neoplasm; 4) normal peristalsis; 5) good vascularization; 6) histographic index I=0.32; 7) strain ratio in sonoelastography SR=2.9.
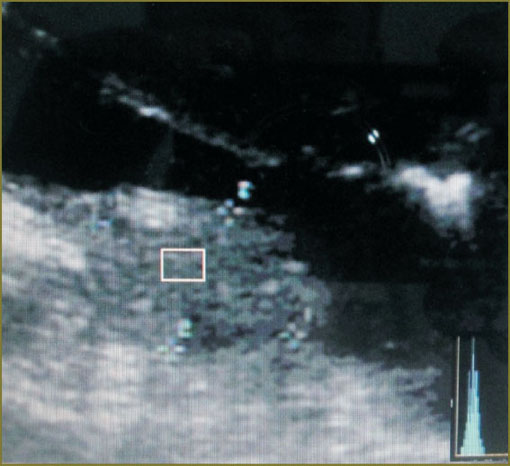 Fig. 5. Sonohistogram of patient К. Gastric leiomyoma Fig. 5. Sonohistogram of patient К. Gastric leiomyoma
|
3. Female patient N., aged 39, with gastric fibrolipoma (Fig. 6). Ultrasonographic signs: 1) clear regular contours; 2) low echogenicity; 3) homogeneous structure; 4) preserved mucosa; 5) normal peristalsis; 6) low vascularization; 7) histographic index I=0.31; 8) strain ratio in sonoelastography SR=0.79.
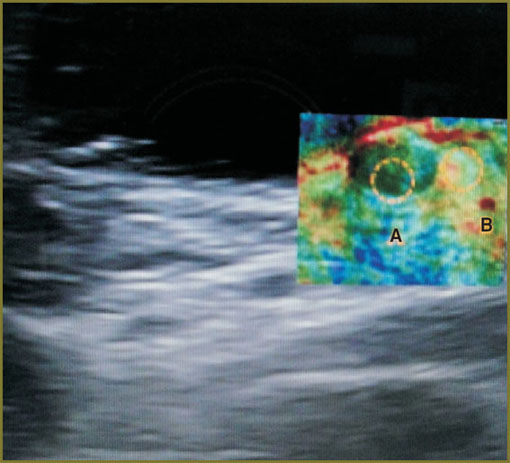 Fig. 6. Sonoelastogram of patient N. Gastric fibrolipoma. А — fibrolipoma elasticity, В — gastric wall elasticity Fig. 6. Sonoelastogram of patient N. Gastric fibrolipoma. А — fibrolipoma elasticity, В — gastric wall elasticity
|
4. Female patient М., aged 59, with gastric endophytic carcinoma (Fig. 7). Ultrasonographic signs: 1) clear irregular contours; 2) low echogenicity; 3) heterogeneous structure; 4) mucous layer is deformed, thin; 5) dysperistalsis; 6) good vascularization, RI=0.45; 7) histographic index I=0.25; 8) strain ratio in sonoelastography SR=10.9.
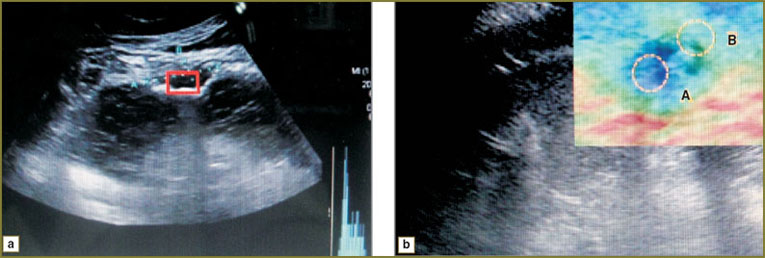 Fig. 7. Sonohistogram (а) and sonoelastogram (b) of patient М. Gastric endophytic carcinoma. А — elasticity of endophytic carcinoma area, В — elasticity of intact gastric wall Fig. 7. Sonohistogram (а) and sonoelastogram (b) of patient М. Gastric endophytic carcinoma. А — elasticity of endophytic carcinoma area, В — elasticity of intact gastric wall
|
5. Patient V., aged 72, with gastric lymphoma (Fig. 8). Ultrasonographic signs: 1) clear contours; 2) low echogenicity; 3) homogeneous structure; 4) mucous layer is preserved; 5) normal peristalsis; 6) low vascularization; 7) histographic index I=0.23; 8) strain ratio in sonoelastography SR=5.6.
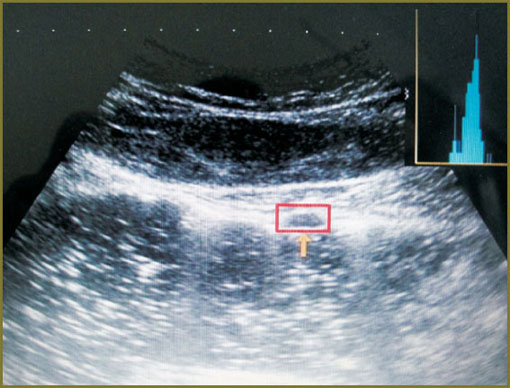 Fig. 8. Sonohistogram of patient V. Gastric lymphoma Fig. 8. Sonohistogram of patient V. Gastric lymphoma
|
The investigations showed that qualitative parameters of ultrasonographic signs of gastric submucous masses do not always enable to define the presence of malignant transformation. Gastric submucous infiltrates of ulcerative or cancerous origin, lymphomas and aberrant (ectopic) pancreas, are the most difficult for differential diagnosis. Only in some cases the type and character of submucous mass vascularization (“mosaic” vascularization) give evidence of possible malignant transformation.
Histographic index (I) and strain ratio (SR), besides resistance index (RI), of arterial vessels of tumors appeared to be the most informative ones from quantitative parameters of ultrasonographic signs of gastric submucous masses. RI was found to be significantly decreased (RI=0.46±0.03; p<0.01) in arterial vessels in endophytic gastric carcinomas (See also [9]). A table shows the diagnostic findings of gastric submucous masses with histographic index and strain ratio values.
The table shows histographic index I and SR in gastric submucous ulcerative infiltrates to differ significantly from similar indices in gastric submucous endophytic carcinomas. The lower value of histographic index in gastric benign submucous tumors was 0.29±0.09, in gastric endophytic carcinomas the index equaled 0.25±0.05. SR values were maximal in gastric endophytic carcinomas, and minimal — in gastric submucous lipomas. Thus, there is a clear downward change of histographic index and strain ratio growth in gastric malignant submucous neoplasms.
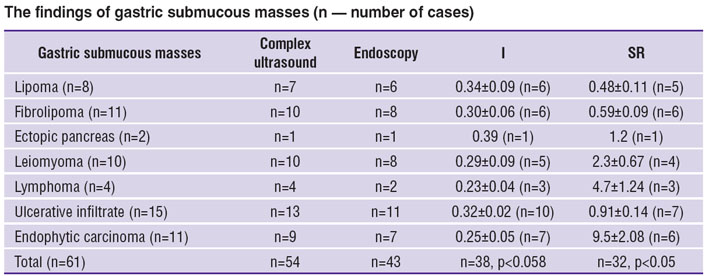 The findings of gastric submucous masses (n — number of cases) The findings of gastric submucous masses (n — number of cases)
|
A graph (Fig. 9) displays a comparative analysis of diagnostic techniques of gastric submucous tumors. The findings strongly suggest that a combined use of complex echography with modern technologies and endoscopy will contribute to significant improvement of study efficiency.
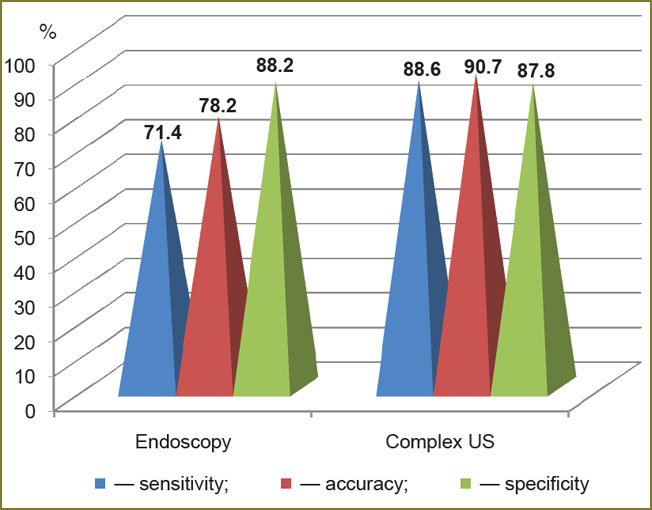 Fig. 9. Comparative analysis of diagnostic techniques of gastric submucous masses Fig. 9. Comparative analysis of diagnostic techniques of gastric submucous masses
|
Conclusion. Modern ultrasound technologies — sonoelastography and amplitude sonohistography — enable to determine effectively the density and elasticity of gastric submucous tumors that contributes to more qualitative differential diagnosis and appropriate modality development. In malignant gastric submucous tumors, histographic index (I) values are significantly decreased and strain ratio (SR) values are significantly increased. Combined application of complex echography and endoscopy increases diagnostic sensitivity, accuracy and specificity of gastric submucous tumors.
Study Funding and Competing Interest. This study was not supported by any financial sources and there is no topic specific conflict of interest related to the authors of this study.
References
- Starkov Yu.G., Solodinina E.N., Shishin K.V., et al. Endoskopicheskaya diagnostika i lechebnaya taktika pri podslizistykh novoobrazovaniyakh verkhnikh otdelov zheludochno-kishechnogo trakta [Endoscopic diagnosis and management in upper gastrointestinal submucous masses]. Khirurgiya. Zhurnal im. N.I. Pirogova — Surgery. Journal named after N.I. Pirogov 2011; 2: 15–20.
- Bulganina N.A. Diagnosticheskaya konveksnaya endosonografiya pri zabolevaniyakh verkhnikh otdelov zheludochno-kishechnogo trakta. Avtoref. dis. … kand. med. nauk [Diagnostic convex endosonography in upper gastroenterological diseases. Abstract for Dissertation for the degree of Candidate of Medical Science]. Moscow; 2010.
- Perfil’ev I.B. Sovremennye metody endoskopicheskoy diagnostiki i lecheniya neyroendokrinnykh opukholey zheludka. Avtoref. dis. … kand. med. nauk [Modern methods of endoscopic diagnosis and treatment of gastric neuroendocrine tumors. Abstract for Dissertation for the degree of Candidate of Medical Science]. Moscow; 2012.
- Zubarev A.R., Fedorova V.N., Demidova A.K., et al. Ul’trazvukovaya elastografiya kak novaya stupen’ v differentsial’noy diagnostike uzlovykh obrazovaniy shchitovidnoy zhelezy: obzor literatury i predvaritel’nye klinicheskie dannye [Ultrasound elastography as a new step in differential diagnostics of nodal thyroid masses: review and preliminary clinical findings]. Meditsinskaya vizualizatsiya — Medical Imaging 2010; 1: 1–6.
- Giovannini M. Endoscopic ultrasound elastography. Pancreatology 2011; 11(Suppl. 2): 34–39, http://dx.doi.org/10.1159/000323496.
- Ryoji Miyahara, Yasumasa Niwa, Masanao Nakamura, et al. Endoscopic ultrasound elastography for the upper gastrointestinal tract disease. In: Digestive Disease Week, May 17th–22nd, 2008. San Diego, USA; 2008.
- Dietrich C.F. Real-time tissue elastography. Multiple clinical applications. Multiple clinical solutions. Endoskopie Heute 2011; 24: 177–212.
- Zubarev A.V., Gazhonova V.E., Khokhlova E.N., et al. Elastografiya — novyy metod poiska raka razlichnykh lokalizatsiy [Elastography — a new search technique of various tumor localizations]. Radiologiya – Praktika — Radiology – Practice 2008; 6: 6–18.
- Mikhaylov M.K., Tukhbatullin M.G. Kompleksnaya luchevaya diagnostika opukholey zheludka [Complex radiodiagnosis of gastric carcinomas]. Kazan: FEN; 2001.









