Evolution of Bioreactors for Extracorporeal Liver Support
The development of effective extracorporeal liver support systems in acute and chronic hepatic failure for transplantology purposes and in toxic injuries is a promising direction in modern biomedical studies. Widely used techniques are based on physicochemical interactions of biological molecules, and able to perform a detoxification function only (hemodialysis, hemofiltration, hemodiafiltration, sorption, albumin dialysis, plasmapheresis). However, support systems combining both blood/plasma perfusion and cellular technologies to maintain metabolic, synthetic and regulatory hepatic functions — “artificial liver” systems — are being extensively developed in recent decades. The review describes the main types of cell lines cultured to occupy bioreactors, various technological concepts for bioreactor design (dynamic, static), scaffold-carriers as part of bioreactors (structure, biochemical composition). The study gives metabolic characteristics of a cellular component of “bioartificial liver”: nourishment, oxygen saturation. Various types of existing extracorporeal support systems, their evolution, and preclinical and clinical test results are presented.
One can find basic knowledge of liver and hepatic vessels as far back as in ancient literature. A prominent Roman physician and philosopher C. Galenus (131–211) studied liver functions and structure. A. Vesalius (1514–1564) made a major contribution to human anatomy development. The works of F. Glisson (1597–1677), Professor of Medicine and Anatomy in Cambridge, a follower of W. Harvey, are worth mentioning. Studying cardiac anatomy and vessel topography, he was the first who described a capsule covering the liver, and since that time it has been called Glisson’s capsule. F. Glisson is the author of “Anatomia hepatica” published in 1654, in which he first represented in detail liver structure. The works of Н. Rex (1888) and G. Cantlie (1897) were of great importance for liver architectonics understanding. Significant contribution to the study of its structure belongs to C. Couinaud (1922–2008). The idea of segmental division of liver and bile ducts he revised and proposed in 1954 is the basis of surgical hepatology to the present day. Currently, there is a branch of science studying hepatic pathology — hepatology — due to its specific character. Despite a long history of liver structure and functioning study, to the present time a lot of functional and regeneration phenomena of this organ still remain unknown.
Liver has many vital functions, mainly detoxification and synthetic ones. Moreover, due to its detoxification activity, in many diseases liver is a target organ. The severity of clinical manifestations of congenital and acquired hepatic diseases depends on the degree of hepatic parenchymal damage and the capability of intact hepatocytes and stem cells to compensate the loss by proliferation. The decreased liver functional activity lower than critical level results from hepatic insufficiency, which gradually causes severe nervous and metabolic disorders and finally leads to death [1]. Unlike the heart, lungs and kidneys, which have a single primary function, the liver has many vital functions of the body: carbohydrate and fat metabolism, protein synthesis, metabolism of amino acids, ureapoiesis, biotransformation of medicines and toxins, elimination of protein, lipid and pigment metabolic waste products [2]. In contrast to the heart and lungs, now the liver remains probably the only organ, the functions of which have not yet been successfully replaced by artificial support.
Due to tremendous upgrowth of liver surgery in the last two decades there have been determined many stimulation and suppression mechanisms of liver regeneration potential, as well as those of hepatic failure. A steadfast rule of surgical hepatology is leaving at least a patient’s 1% liver mass of body mass. In case of liver fibrosis or cirrhosis, the percentage is to be doubled or tripled depending on parenchyma damage degree. The smaller post-resection fragment does not regenerate, and the condition is interpreted as a “small-for-size syndrome” and results in fatal post-resection hepatic failure. For liver failure prevention, over the last 10 years there have been suggested the technologies of controlled stimulation of perspective liver fragment hypertrophy in patient “in situ”. The most frequently used technologies are segmental portal embolization of lobar branch of portal vain (the most affected hepatic lobe) resulting in hypertrophy of contralateral lobe parenchyma; it is possible to combine it with occlusional embolization of the appropriate artery. ALPPS (Associating Liver Partition and Portal vein Ligation for Staged hepatectomy) is the most effective technology, which enables to achieve the increase of perspective parenchyma volume by 78.4% and more over 7–9 days [3, 4].
Currently, liver transplantation is the most effective and practicable treatment method for acute post-resection and progressive chronic liver failure. There have been performed whole liver transplantations from a deceased donor or partial liver transplantations when a liver part is taken from a live relative counting on liver hypertrophy in a postoperative period.
And liver transplantation availability is limited both in Russia and abroad. According to the studies of the last 10 years [5], one in three patients does not live till transplantation, mainly due to the shortage of donor organs and a time consuming search process of a matched donor.
In order to reduce death rate among patients with hepatic failure there have been developed effective extracorporeal livers supports used before transplantation.
Physicochemical liver support systems
In recent times, in clinical practice there have been used the following separate or combined methods for artificial liver replacement: diffusion (hemodialysis), convection (hemofiltration), diffusion-convectional (hemodiafiltration), sorption (LPS-sorption — sorption of lipopolysaccharide toxines, plasmosorption), diffusion-convection-sorption (albumin dialysis) and afferent (plasmapheresis) [5, 6]. All the listed methods are based on the usage of physicochemical interactions of biological molecules, and low- and medium-weight uremic toxins, small proteins, some bacterial endotoxins are eliminated from patient’s plasma.
A modified system of fractional plasma separation and adsorption — Prometheus (Fresenius Medical Care, Germany) provides an example of one of known and widely-accepted detoxification systems. Prometheus system consists of dialysis machine with an integrated module for albumin separation and adsorption. The system eliminates albumin-bound and water-soluble toxins that making hepatocyte regeneration easier [7]. In addition, in Germany there has been developed and widely used MARS — a molecular absorbing recirculating system (a molecular system of recirculating absorption), which eliminates water-soluble and albumin-bound toxins. MARS has been used in clinical practice since 1993. It is worth noting that apparatuses and consumables are high-cost (several thousand dollars per a procedure) that limits widespread application of these systems [8]. In Russia only a few clinics are equipped with such systems for temporary liver support.
All mentioned physicochemical systems for extracorporeal liver support aim at maintaining patients with liver failure within a short period of time determined by the severity of hepatic insufficiency.
The common disadvantages are the following:
1) lack of nervous and humoral regulation mechanisms, as well as the connection with other body organs and systems;
2) insufficiency of detoxification capacity to cease liver parenchyma damage [9].
Nevertheless, if liver functions are to be supported, the existing blood purification systems are the only techniques to support a patient before transplantation.
In 1991 for the first time there was introduced Auxiliary partial orthotopic liver transplantation (APOLT) — the technology of temporary liver transplantation (replating) without removal of genuine damaged and partially necrotized liver [10, 11]. The technique is based on regeneration of proper liver for about 4 weeks in fulminant hepatic failure. The success results from complete substitution of hepatic function in this period. In proper organ restoration established by control morphological examinations of bioptic material, transplanted donor liver is removed and transplanted to the next recipient — “domino effect” [12]. Despite the exoticism of the technique, it demonstrates high efficiency [13]. Limiting factors of APOLT: the technique is used in highly specialized medical centers with unique surgical equipment. Unfortunately, the method has not found its application in world practice.
Since liver functions include not only detoxification, an ideal extracorporeal system should also support metabolic, synthetic and regulatory hepatic functions [14, 15]. In this regard, since the 80s of XX century the support systems combining blood/plasma perfusion and cell technologies have being extensively developed.
“Bioartificial liver” and extracorporeal liver support
“Artificial liver” bioreactor structure. Currently, there are liver support systems using living hepatocyte cultures — “artificial liver” bioreactors. Technology concepts in bioreactor structure are various [16]. In general, a bioreactor can be defined as a large closed system, inside which there are two main parts: cell activity zone and plasma and blood circulation zone separated by a semi-permeable membrane. After systemic blood purification (detoxification, dialysis) patient’s plasma or blood enters a bioreactor, where hepatocytes enrich them by synthesis products. From plasma hepatocytes take oxygen, nutrients and toxins, while bile acids, blood coagulation factors, lipoproteins, aminoacids and other metabolism products of hepatocytes return to plasma. A membrane is a barrier for large-mass substances (transport protein, immunoglobulins, lipoproteins), and for immune-competent human blood cells. Substances can be transported by diffusion or convection, as well as by concentration gradient, it depending on membrane’s charge, size, and physicochemical properties [17] (Fig. 1). Inside the cell activity zone, oxygen, nutrients, toxins, waste products of hepatocytes are transported by diffusion [18, 19].
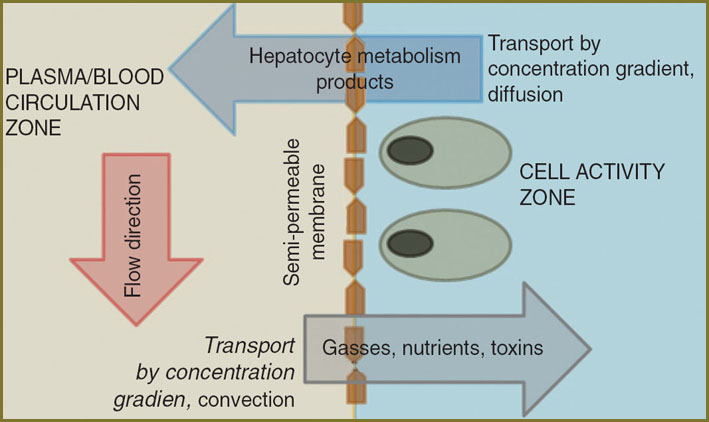 Fig. 1. A bioreactor model Fig. 1. A bioreactor model
|
Cell cultures as part of a bioreactor. Now the main efforts of researchers are focused on the development of appropriate cell lines, and arrangement of optimal conditions for their culture as part of a bioreactor. A cell metabolism characteristic is a topic of interest for many studies, since cells should match some criteria for efficient implementation of bioregulating and synthetic functions:
1) to perform functions of normal hepatic cells (detoxification, synthesis of biologically active substances);
2) to be able to proliferate actively (to reach minimum volume, up to 400 g) biomasses in bioreactor;
3) to function under the conditions of constant contact with plasma of patients with acute hepatic failure [20].
There are several approaches to develop efficient cell lines as part of a bioreactor.
1. The use of allergenic primary hepatocytes isolated from donor tissues [21, 22]. In order to increase the life time of adult donor’s hepatocyte, some researchers describe in their studies hepatocyte treated by biologically active substances, in particular, immunosuppressants FK506 and cyclosporine А [23].
2. The use of xenogeneic, of animal origin, primary hepatocytes. Primary porcine hepatocytes are really used in the overwhelming majority of liver support systems [24, 25]. The choice is explained by the lack of human hepatocytes, similarity of human and porcine hepatocytes, the availability of porcine hepatocytes. However, the use of porcine hepatocytes has a certain risk. According to Food and Drug Administration (FDA, USA) guidelines, only certain pigs bred in appropriate conditions should be used for porcine hepatocytes applied as cell lines [26]. It relates mainly to the problem of eventual immune response in patients after their blood perfusion through xenohepatocytes. Another important issue is the problem of protection of porcine hepatocytes against potentially active factors of patients’ immune system during perfusion. Moreover, despite hepatic functions in all mammals are similar, there are still differences, and xenogeneic hepatocytes cannot perform all metabolic task complex of a human liver [27].
3. The use of immortal and genetically modified human and animal hepatocyte lines [28]. This field now is the most prospective [29]. Such cells are characterized by unlimited but controlled division property, minimum risk of infection transmission, and they possess the main biological characteristics and functions of primary hepatocytes [30]. Various immortalized cell lines of hepatocytes are used for cell culture in a bioreactor: PICM-19 line was developed from 8-day porcine embryonic cells [31], there were developed human immortalized lines of hepatocyte-like cells — HepZ [32], HepG2 [33], cBAL111 [34]. In addition, Chang Liver developed in 1954 is used, though the line supposedly isolated from tumor cells, has limited application due to its oncogenic potential [35].
All the mentioned methods of making specialized monocultures have one characteristic: when they are used, the lack of hepatocyte growth stimulation causes the limitation on the number of proliferation cycles — up to eight [36]. It prevents from obtaining a sufficient number of normal hepatocytes to fill a bioreactor. Moreover, besides hepatocytes, a healthy liver also has other cells, which stimulate their proliferation and differentiation (Kupffer cells, stelate cells) [37], but they are not used in these techniques.
However, there have been carrying on the studies concerned with the use of originally different cells in a bioreactor, as well as the application of combined culture of several cell types [38]. In such researches both specialized and pluripotent cells are used as co-cultures. An experimental work [39] has showed that simultaneous culture of porcine hepatocytes with non-parenchymal (duct, stellate, and endothelial cells) human cells in matrigel results in spontaneous formation of microsinusoids expressing albumin and cytochromes Р450, as well as micro-tissue structures — progenitors of bile ducts and blood vessels. Co-cultivation of human primary hepatocytes with endothelial cells of bile ducts was found to have a favorable effect on both hepatic cell lines and stimulate active hepatocyte functioning [40, 41]. The researches on co-culture of primary human hepatocytes and multipotent bone marrow mesenchymal cells [42, 43] have shown that hepatocytes cultured under such conditions have higher synthetic and proliferative potential.
One more method of hepatocyte-like cell culture is the use of stem cells of various origin. Controlled differentiation of marrow bone and adipose tissue-derived stroma cells was found to enable to culture committed hepatic cells. For such differentiation, fibroblast growth factor FGF1 [44], hepatocyte growth factor HGF [45], specialized differentiation media are used [46]. To cultivate hepatocyte-like cells there also used progenitor hepatic cells, which are precursors of hepatocytes and bile duct cells [47].
However, some studies describe the differentiation of stromal stem cells into hepatocyte-like cells to be due to the use of biologically active carrier-material. In particular, the use of rat decellularized liver as a 3D framework for cell growth has showed that such a biotemplate stimulates target differentiation of mesenchymal stem cells in mature hepatocytes regardless of growth factors in cultural medium [48].
Metabolic characteristics of cells as part of a bioreactor. In vivo hepatic cells are in want of nutrients, oxygen and highly sensitive to metabolite concentration changes. Therefore, it is crucial to create conditions close to natural in a bioreactor.
Nourishment. In vivo cells are nourished through an extensive capillary network. The distance between capillaries and cells is not long, and oxygen and nutrients penetrate the cells by diffusion. An artificial system lacks such a capillary network. It results in non-regular distribution of culture medium inside cell mass, and substances synthesized by hepatocytes cannot completely be transported to patient’s blood [49]. The problem is solved in a variety of ways, e.g. hepatocyte cultivating on different permeable substrates [50], as well as by constant stirring of culture media [51].
Oxygen saturation. Oxygen enters culture from gaseous layer above the media surface, and its entrance is limited by solubility coefficient, which is rather low. Under conditions of high cell density, only a few cells are in direct contact with phase boundary surface and can receive oxygen by diffusion [52]. Inside cell mass, where cells are in contact with each other only, oxygen does not pass from cell to cell leading to acute hypoxia. The problem is settled by various means. One of the variants is medium stirring, when oxygen is transferred by diffusion and by convection [53]. In some bioreactor models access of oxygen to cells is increased due to additional oxygen sources, and in other bioreactors — direct oxygenation of culture medium, or plasma or whole blood is used [54]. In the latter case, separate ways of oxygenation inside a bioreactor are provided.
Scaffolds. Cells inside a bioreactor are usually attached to some carrier substituting extracellular matrix [55]. In addition, cell culture in 3D space rather than a classical monolayer is used that contributes to differentiation, intercellular contact formation, and the higher cell viability [56]. Cell substrates, or scaffolds, can be various in form and material.
1. Scaffolds from natural materials (collagen, alginate, fibronectin, gelatin, matrigel). Their advantage is in the effective cell bonding and their further proliferation. However, strength of natural materials is insufficient, and their micro-architecture is difficult to simulate [57].
2. Scaffolds from biocompatible synthetic materials. Among these are aliphatic polyether-based polymers: polylactide, polyglycolide, their co-polymers and polycaprolactone, synthetic polypeptides [58], glass [59]. Synthetic scaffolds are stronger; they can be formed in accordance with use requirements of a particular cell line [56].
3. Scaffolds from a mixture of natural and synthetic materials. As a rule, polycaprolactone and collagen are used [60], and other components: alginate and chitosan are added [61].
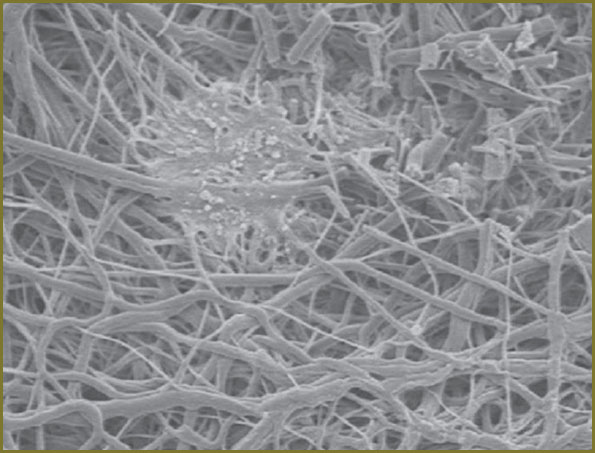
Suitable topological, morphological and biochemical conditions should be provided for cell attachment and proliferation [62]. Cell expansion on a scaffold depends on cell distribution rate, as well as penetration rate of cells into pores (external and internal transport) [63, 64]. And if outside transport depends primarily on carrier material, inside transport depends on pore-cell size ratio [65]. The following scaffold groups are the most frequently used: group 1 consists of thin (2–3 mm thick) plates or discs with porous surface (Fig. 2). Hepatocytes cultured on such a surface colonize pores forming clusters. The second group represents hollow membrane fibers, in which hepatocytes are cultured on the internal surface. The studies of last years have reported nanofibers made of natural and artificial polymers to be used [66]. Such fibers are clustered in 3D structures (Fig. 3) by various techniques, among which electrospinning gains its popularity [67]. Moreover, incapsulation technique (hepatocytes are encapsulated, capsules being made of photopolymerized hydrogels) is used to make scaffolds [68].
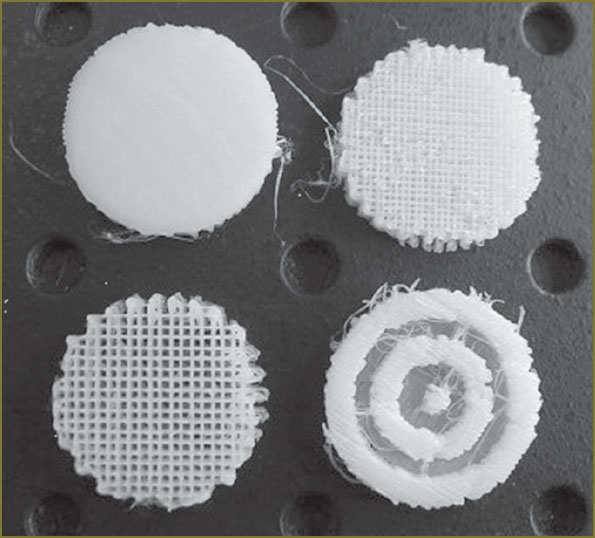 Fig. 2. The appearance of disc polymer polylactide scaffolds [56] Fig. 2. The appearance of disc polymer polylactide scaffolds [56]
|
|
|
The use of several cell cultures as a part of a bioreactor, can promote hepatocyte functioning improvement. For example, the use of fibroblasts 3T3-J2 as a feeder layer results in increased urea and albumin secretion by hepatocytes [69]. Experiments have showed hepatocytes to be able both to adhere to the material surface, and self-organize into clusters [70]. And when hepatocytes and endothelial cells are co-cultured, micro-vessels and capillaries form simulating liver tissue [40]. Therefore, when creating fabric-engineering constructions, the interaction between various cells should be taken into consideration.
Bioreactor design. Effective bioreactor functioning requires optimization of transport of nutrients and metabolites to cells, on the one hand, and delivery system of plasma to hepatocytes — on the other hand. If this goal is achieved, some technical problems arise, which are solved differently in different bioreactors [71]. All bioreactor designs can be divided into two large groups — static and dynamic.
In static bioreactors (Fig. 4) cells (single [72] or organized into spheroid structures [73, 74]) are cultured on scaffold surface, where they subsequently penetrate inside under the action of gravity and capillary force. Scaffolds with cells are washed by medium and surrounded by semi-permeable membrane, through which metabolites are exchanged. Plasma or blood flow washes membrane enabling oxygen, nutrients and toxins to penetrate into hepatocytes; and cell metabolism products enter plasma or blood [75, 76].
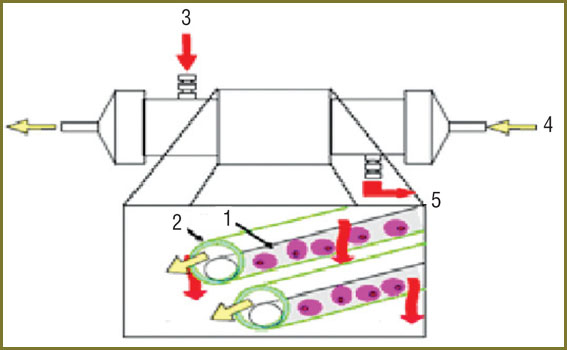
In dynamic bioreactors (Fig. 5) cells are also cultured on scaffolds surrounded by a semi-permeable membrane, outside which there is plasma or blood flow, and then the whole systems starts working. Magnetic stir bars or a rotating housing are used. Scaffold rotation results in better distribution of cells inside scaffolds, cells coming through pores and filling all work space in a scaffold. It contributes to higher cell proliferation and increase of cell life [27, 67]. In addition, due to constant rotation, cells are better washed by culture medium, and metabolite exchange between patient’s plasma or blood and hepatocytes is more effective [2]. As a result, cells have no hypoxia and nutrient lack. Most modern bioreactors are dynamic.
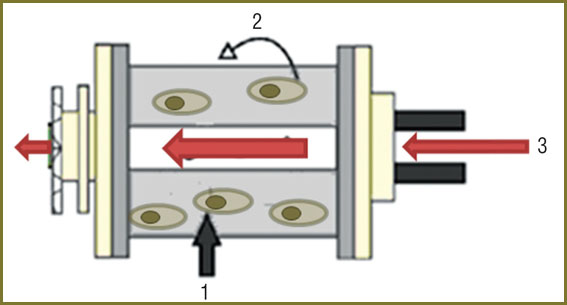 Fig. 5. Diagram of a dynamic bioreactor [35]: 1 — aggregates of hepatocytes; 2 — housing rotation direction; 3 — direction of incoming plasma or blood flow Fig. 5. Diagram of a dynamic bioreactor [35]: 1 — aggregates of hepatocytes; 2 — housing rotation direction; 3 — direction of incoming plasma or blood flow
|
Variety of bioreactor technologies. By now, several clinical studies have been carried out and only a preliminary estimation of success and further prospects can be made. Basic bioreactor construction types of “artificial liver” are given in a Table.
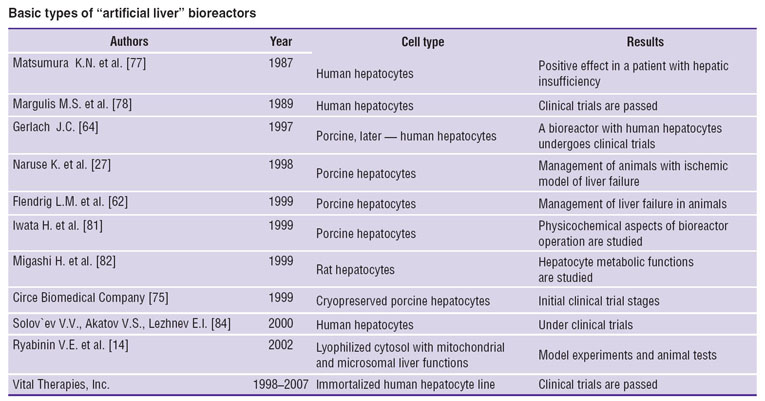 Basic types of “artificial liver” bioreactors Basic types of “artificial liver” bioreactors |
The first report on bioartificial liver use in clinical practice published in 1987 by K.N. Matsumura et al. [77] described a positive effect in patients with liver failure due to bile duct carcinoma. The device used consisted of a dialyzer plate with highly-permeable cellophane membranes with hepatocytes immobilized. At that time a group headed by M.S. Margulis [78] performed a clinical trial of artificial liver on patients with acute hepatic failure. A bioreactor was composed of a column with activated carbon and suspension of hepatocytes held by a nylon filter. Patient’s blood was perfused through the system for about 6 h, a column was changed every 24 hours, since suspension of single cells quickly lost its metabolic activity.
In 1997 J.C. Gerlach [64] described a complex four-component bioreactor based on hollow membrane fibers, the collocation of which looked like a model of natural vasculature. Three-dimensional construction included semi-permeable membrane fibers organized as 2D-structures. Regular elements of the network were three hydrophilic fibers, two of which were colonized by cells, and the third was designed for oxygen supply and carbon dioxide removal. Porcine or human parenchymal and non-parenchymal hepatic cells were cultured on the outer part of fibers. Plasma entered the lumen of membrane bundles, was filtered, after that it washed the cells and returned to a patient. For this reactor there was adjusted a high cell viability and the effective use of available cell mass [79]. Such a bioreactor cultured by human hepatocytes was approved for clinical trials, though there is no information on success test results.
K. Naruse et al. in 1998 [27] described the device based on primary porcine hepatocytes fixed on a polyester matrix. The system was characterized by preliminary formation of matrix cylindrical membrane and the following direction of blood flow, which is beyond the membrane, towards its internal part in a radial reactor. External oxygenation was performed for sufficient oxygen supply of hepatocytes. The application of the technique enabled to increase survival rate of pigs with ischemic model of liver failure.
In 1999 Flendrig L.M. et al. [62] suggested another bioreactor type, in which porcine hepatocytes were cultured being fixed to spiral fibers made of polyester non-woven fabric forming 3D network. The construction was packed in acylindric acrylic case. Inside the case there was the perfusion of plasma flowing along a bioreactor. Between adjacent layers there were inserted microporous membranes for oxygen saturation and carbon dioxide removal. Moreover, hepatocytes were recorded to form aggregates, and so, such a bioreactor construction resembled a natural hepatic unit.
S. Naka et al. in 1999 [80] developed a system based on primary porcine hepatocytes. In this bioreactor hepatocytes came in contact with plasma through polysulphone membranes. In addition, primary porcine hepatocytes in collagen gel were placed in capillary limens, while blood was perfused through extraluminal space. In this way an additional substance flow was arranged and the necessary conditions for hepatocyte functioning were provided. Since collagen is polymerizable, there was polymerizing reduction of gel amount and channelization in lumens of fibers, through which culture medium was circulating. The bioreactor was successfully tested on animals, and now clinical trial results are forthcoming.
Н. Iwata et al. also in 1999 [81] developed a similar system and published their research findings describing the kinetics of hepatocyte metabolic reactions, the hepatocytec being cultured on a cartridge with extraluminal space.
Later in 1999, H. Migashi et al. [82] in their study used hepatocyte culture fixed on polyvinylformaldehyde resin matrix. Cubical-shaped material with fixed primary rat hepatocytes was placed in a special column. The studies showed rather long-term (up to 12) maintenance of hepatocyte metabolic functions.
Circe Biomedical Company in Hepat Assist devices used cryopreserved primary porcine hepatocytes fixed to collagen-coated dextran particles [75]. There were reported initial test phase data on these devices in 2000 (treatment experience of 39 patients with hepatic insufficiency), but nothing was said about their success [83].
In 2000 a group of Russian researchers [84] patented “a bioartificial liver”, a column bioreactor consisting of a tank filled by particles of a neutral carrier and hepatocytes. Glass balls 1–3 mm in diameter were used as carrier’s particles. They create a 3D matrix, in which multicellular hepatocyte aggregates are formed and withheld in free spaces between the particles. Biological fluid is perfused through a column downwards and directly washes cell aggregates distributed by a carrier throughout the reactor. At present the reactor undergoes clinical trials.
A “bioartificial liver” system developed in Chelyabinsk under the charge of Prof. V.Е. Ryabinin, which has undergone model experiments and animal tests, is of interest [14]. The principle of operation of the bioreactor is in the usage of a semi-permeable membrane. The technique contributes to the contact of patient’s blood and a contour containing special biological solution developed by V.Е. Ryabinin — lyophilized cyosol with microsomal and mitochondrial hepatocyte fraction. It should be emphasized that the systems uses not hepatocytes but their organelles and significantly differs from bioreactors with cellular components.
Currently, in clinical practice ELAD (Vital Therapies, Inc., USA) is used. It has passes clinical trials successfully and based on immortalized line of human hepatocytes, which are fixed and grow in extracapillary space of a dialyzer with semi-permeable membrane made of polysulphone [9]. Patient’s blood enters ELAD from the jugular vein through a catheter. In the device plasma is separated and directed in dialyzers containing about 440 g of living cells. The device is developed aiming to provide continuous liver support for the period of 30 days in patients with acute or fulminant hepatic failure. The system serves to provide liver function retention, sustain patient’s life and protect nervous system against toxins before transplantation.
Conclusion
Two decades have passes since the first bioreactors have appeared. Many technologies have been developed, and cell culture approaches have been improved over this period of time. There have been developed systems, which have undergone clinical trials, and there is a system used in clinical practice. However, many problems in the sphere of cell technologies concerning the increase of hepatocyte culture life still remain unsolved. To increase the period of hepatocyte function retention numerous researches are being carried on, they aim at developing bioactive matrixes. New engineering solutions applicable to cell supply of oxygen and nutrients are being developed. In the long term, there is probability that a “bioartificial liver” system will be used in the management of chronic hepatic diseases like an artificial kidney apparatus used in renal disorders.
Study Funding. The work was supported by Russian Foundation for Basic Research project No.13-04-97141 “Study of functional activity of cell populations of hepatocytes for “Artificial liver” bioreactor development”.
Conflict of Interests. The authors have no conflicts of interests to declare.
References
- Garbuzenko D.V., Popov G.K. Mekhanizmy regulyatsii regeneratsii pecheni [Regulation mechanisms of liver regeneration]. Rossiyskiy zhurnal gastroenterologii, gepatologii, koloproktologii — Russian Journal of Gastroenterology, Hepatology, Coloproctology 2001; 11(1): 21–25.
- Sussman N.L., Kelly J.H. The artificial liver. Sci Am Sci Med 1995; 2(3): 68–77.
- Alvarez F.A., Ardiles V., Sanchez Claria R., et al. Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS): tips and tricks. J Gastrointest Surg 2013; 17(4): 814–821, http://dx.doi.org/10.1007/s11605-012-2092-2.
- Torres O.J., Moraes-Junior J.M., Lima N.C., Moraes A.M. Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS): a new approach in liver resections. Arq Bras Cir Dig 2012; 25(4): 290–292, http://dx.doi.org/10.1590/S0102-67202012000400015.
- Stockmann H.B. Prospects for the temporary treatment of acute liver failure. Eur J Gastroenterol Hepatol 2002; 14: 195–203.
- Sauer I.M., Zeilinger K., Pless G., et al. Extracorporeal liver support based on primary human liver cells and albumin dialysis — treatment of a patient with primary graft non-function. J Hepatol 2003; 39: 649–653.
- Rifai K., Ernst T., Kretschmer U., et al. Prometheus — a new extracorporeal system for the treatment of liver failure. J Hepatol 2003; 39: 984–990, http://dx.doi.org/10.1016/S0168-8278(03)00468-9.
- Jalan R., Williams R. The role of the Molecular Adsorbents Recirculating System (MARS) in the management of liver failure. Perfusion 2004; 19: 43–48, http://dx.doi.org/10.1191/0267659104pf716oa.
- Ellis F.J., Hughes R.D., Wendon J.A., et al. Pilot-controlled trial of the extracorporeal liver assist device in acute liver failure. Hepatology 1996; 24: 1446–1451.
- Gubernatis G., Pichlmayr R., Kemnitz J., Gratz K. Auxiliary partial orthotopic liver transplantation (APOLT) for fulminant hepatic failure: first successful case report. World J Surg 1991; 15(5): 660–665, http://dx.doi.org/10.1007/BF01789221.
- Azoulay D., Samuel D., Ichai P., et al. Auxiliary partial orthotopic versus standard orthotopic whole liver transplantation for acute liver failure: a reappraisal from a single center by a case-control study. Ann Surg 2001; 234(6): 723–731.
- Ringe K.I., Galanski M., Ringe B. From abernethy to APOLT. Liver Transpl 2008; 14(7): 1067–1068, http://dx.doi.org/10.1002/lt.21457.
- Kasahara M., Takada Y., Egawa H., et al. Auxiliary partial orthotopic living donor liver transplantation: Kyoto Univ. experience. Am J Transplant 2005; 5(3): 558–566, http://dx.doi.org/10.1002/lt.20692.
- Ryabinin V.E., Grobovoy S.I., Tkachev S.I., Kravchuk I.E. Issledovanie svoystv tsitozolya pecheni i effektivnosti sposoba ego ispol’zovaniya v apparate “biologicheskaya vspomogatel’naya pechen’” [The study of hepatic cytosolic properties and the efficiency of its use in biological liver assist device]. Vestnik RAMN — Herald of RAMS 2002; 3: 21–24.
- Ryabinin V.E., Suprun V.I., Tkachev S.I. Ispol’zovanie iskusstvennykh sistem zhizneobespecheniya i kletochnykh tekhnologiy pri lechenii zabolevaniy pecheni [Application of artificial life support systems and cellular technologies in hepatotherapy]. Chelyabinsk: Yuzh.-Ural. nauch. tsentr Ros. akad. med. nauk; 2007; 148 p.
- Pless G. Bioartificial liver support systems. Methods Mol Biol 2010; 640: 511–523, http://dx.doi.org/10.1007/978-1-60761-688-7_28.
- Saich R. Toxic molecules in liver failure plasma [dissertation]. London (UK): Univ. of London; 2010.
- Catapano G., Di Lorenzo M.C., Della Volpe C., et al. Polymeric membranes for hybrid liver support devices: the effect of membrane surface wettability on hepatocyte viability and functions. J Biomater Sci Polymer Ed 1996; 7(11): 1017–1027.
- Gerlach J. Development of a hybrid liver support system: a review. Int J Artif Organs 1996; 19(11): 645–654.
- Pan X.-P., Li L.-J. Advances in cell sources of hepatocytes for bioartificial liver. Hepatobiliary Pancreat Dis Int 2012; 11(6): 594–605, http://dx.doi.org/10.1016/S1499-3872(12)60230-6.
- LeCluyse E.L., Alexandre E., Hamilton G.A. Isolation and culture of primary hepatocytes from resected human liver tissue. Methods Mol Biol 2005; 290: 207–229.
- Ryabinin V.E. Ispol’zovanie metodov kletochnoy i efferentnoy terapii pri lechenii pechenochnoy nedostatochnosti [The use of cellular and efferent methods for hepatic failure treatment]. Vestnik transplantatsii iskusstvennykh organov — Vestnik of Artificial Organ Transplantation 2002; 1: 42–49.
- Yokoyama I., Hayakawa A., Hayashi S., et al. Fas antigen expression of hepatocytes and its modification by immunosuppressants. Dig Dis Sci 1997; 42(12): 2471–2475.
- Chen Z., Ding Y., Li G. Configuration of a new bioartificial liver support system and in vitro evaluation of its functions. Ann Clin Lab Sci 2005; 35(1): 7–14.
- Naik S., Trenkler D., Santangini H. Isolation and culture of porcine hepatocytes for artificial liver support. Cell Transplant 1996; 5(1): 107–115, http://dx.doi.org/10.1016/0963-6897(95)02003-9.
- PHS guideline on infectious disease issues in xenotransplantation. U.S. Food and Drug Administration; 2001. http://www.fda.gov/biologicsbloodvaccines/guidancecomplianceregulatoryinformation/ guidances/xenotransplantation/ucm074727.htm.
- Naruse K., Nagashima I., Sakai Y., et al. Efficacy of a bioreactor filled with porcine hepatocytes immobilized on nonwoven fabric for ex vivo direct hemoperfusion treatment of liver failure in pigs. Artif Organs 1998; 22(12): 1031–1037.
- Priesner C., Hesse F., Windgassen D., et al. Liver-specific physiology of immortal, functionally differentiated hepatocytes and of deficient hepatocyte-like variants. In Vitro Cell Dev Biol 2004; 40: 318–330, http://dx.doi.org/10.1290/0404031.1.
- Kuge H., Ohashi K., Yokoyama T., et al. Genetic modification of hepatocytes towards hepatocyte transplantation and liver tissue engineering. Cell Transplant 2006; 15(1): 1–12.
- Matsumura T., Takesue M., Westerman K.A., et al. Establishment of an immortalized human-liver endothelial cell line with SV40T and hTERT. Transplantation 2004; 77(9): 1357–1365.
- Sussman N.L., Chong M.G., Koussayer T., et al. Reversal of fulminant hepatic failure using an extracorporeal liver assist device. Hepatology 1992; 16: 60–65, http://dx.doi.org/10.1002/hep.1840160112.
- Werner A., Duvar S., Müthing J., et al. Cultivation of immortalized human hepatocytes HepZ on macroporous CultiSpherG microcarriers. Biotechnol Bioeng 2000; 68(1): 59–70.
- Hsieh S., Lin P.-Y., Hsieh C.-W., et al. Probing the adhesion of hepatocellular carcinoma HepG2 and SK-Hep-1 cells. J Chin Chem Soc 2012; 59: 929–933.
- Deurholt T., van Til N.P., Chhatta A.A., et al. Novel immortalized human fetal liver cell line, cBAL111, has the potential to differentiate into functional hepatocytes. BMC Biotechnol 2009; 9: 89–104, http://dx.doi.org/10.1186/1472-6750-9-89.
- Talbot N.C., Caperna T.J., Wells K.D. The PCM-19 cell line as an in vitro model of liver bile ductules: effects of cAMP inducers, biopeptides and pH. Cells Tissues Organs 2002; 171(2–3): 99–116, http://dx.doi.org/10.1159/000063704.
- Celton-Morizur S., Desdouets C. Polyploidization of liver cells. Adv Exp Med Biol 2010; 676: 123–35.
- Yarygin K.N. Regeneratsiya organov i tkaney: ierarkhicheskaya i stokhasticheskaya modeli. V kn.: Tezisy dokladov vserossiyskoy i mezhdunarodnoy nauchnoy konferentsii “Stvolovye kletki i perspektiva ikh ispol’zovaniya v zdravookhranenii” [Organ and tissue regeneration: hierarchical and stochastic models. In: Abstracts of Russian and international scientific conference “Stem cells and prospects for their application in public health service”]. Moscow; 2007; p. 9–11.
- Zhang W., Tucker-Kellogg L., Narmada B.C., et al. Cell-delivery therapeutics for liver regeneration. Adv Drug Deliv Rev 2010; 62: 814–826, http://dx.doi.org/10.1016/j.addr.2010.02.005.
- Soto-Gutierrez A., Navarro-Alvarez N., Yagi H., et al. Engineering of an hepatic organoid to develop liver assist devices. Cell Transplant 2010; 19: 815–822, http://dx.doi.org/10.3727/096368910X508933.
- Garbuzenko D.V. Mekhanizmy kompensatsii struktury i funktsii pecheni pri ee povrezhdenii i ikh prakticheskoe znachenie [Hepatic structure and function compensation mechanisms in liver damage and their practical importance]. Rossiyskiy zhurnal gastroenterologii, gepatologii, koloproktologii — Russian Journal of Gastroenterology, Hepatology, Coloproctology 2008; 18(6): 14–21.
- Gebhardt R. Co-cultivation of liver epithelial cells with hepatocytes. Methods Mol Biol 2002; 188: 337–346, http://dx.doi.org/10.1385/1-59259-185-X:337.
- Mohajerani S.A., Nourbakhsh M., Cadili A., et al. Transplant of primary human hepatocytes cocultured with bone marrow stromal cells to SCID Alb-uPA mice. Cell Medicine 2010; 1: 81–92.
- Yang G.J. Experimental study on the co-culture of hepatocytes with bone marrow mesenchymal stem cells in vitro [dissertation]. Nanjing (JP): Nanjing Medical Univ., 2009.
- Banas A., Teratani T., Yamamoto Y., et al. Adipose tissue-derived mesenchymal stem cells as a source of human hepatocytes. Hepatology 2007; 46: 219–228, http://dx.doi.org/10.1002/hep.21704.
- Jones C.N., Tuleuovaa N., Leea J.Y., et al. Cultivating liver cells on printed arrays of hepatocyte growth factor. Biomaterials 2009; 30(22): 3733–3741, http://dx.doi.org/10.1016/j.biomaterials.2009.03.039.
- Gerbal-Chaloin S., Duret C., Raulet E., et al. Isolation and culture of adult human liver progenitor cells: in vitro differentiation to hepatocyte-like cells. Methods in Mol Biol 2010; 640: 247–260, http://dx.doi.org/10.1007/978-1-60761-688-7_12.
- Xiong A., Austin T.W., Lagasse E., et al. Isolation of human fetal liver progenitors and their enhanced proliferation by three-dimensional coculture with endothelial cells. Tissue Eng 2008; 14: 995–1006, http://dx.doi.org/10.1089/tea.2007.0087.
- Ji R., Zhang N., You N., et al. The differentiation of MSCs into functional hepatocyte-like cells in a liver biomatrix scaffold and their transplantation into liver-fibrotic mice. Biomaterials 2012; 33: 8995–9008, http://dx.doi.org/10.1016/j.biomaterials.2012.08.058.
- Hoekstra R., Chamuleau R.A. Recent developments on human cell lines for the bioartificial liver. Int J Artif Organs 2002; 25(3): 182–191.
- Kazemnejad S. Hepatic tissue engineering using scaffolds: state of the art. Avicenna J Med Biotech 2009; 1(3): 135–145.
- Smith M.D. Techniques for measurement of oxygen consumption rates of hepatocytes during attachment and post attachment. Int J Artif Organs 1996; 19: 36–44.
- Moolman F.S. Oxygen carriers for a novel bio-artificial liver support system [dissertation]. Pretoria (RSA): Univ. of Pretoria; 2003.
- Donato M.T. Characterization of drug metabolizing activities in pig hepatocytes for use in bioartificial liver devices: comparison with other hepatic cellular models. J Hepatol 1999; 31: 542–549.
- Gharravi A.M., Orazizadeh M., Hashemitabar M., et al. Status of tissue engineering and regenerative medicine in Iran and related advanced tools: Bioreactors and scaffolds. Biomed Eng 2012; 5(4): 217–227.
- Willinger M., Schima H., Shmidt C., et al. Microspheres based detoxification system: in vitro study and mathematical estimation of filter performance. Int J Artif Organs 1999; 22: 573–582.
- Leete D.A. Functional design and fabrication of heterogeneous tissue engineering scaffolds [dissertation]. Philadelphia (PA): Drexel Univ.; 2005.
- Koebe H.G. Collagen gel immobilization provides a suitable cell matrix for long term human hepatocyte cultures in hybrid reactors. Int J Artif Organs 1994; 17: 95–106.
- Wang S., Nagrath D., Chen P.C., et al. Three-dimensional primary hepatocyte culture in synthetic self-assembling peptide hydrogel. Tissue Eng 2008; 14(2): 227–236, http://dx.doi.org/10.1089/tea.2007.0143.
- Park J., Li Y., Berthiaume F., et al. Radial flow hepatocyte bioreactor using stacked microfabricated grooved substrates. Biotechnol Bioеng 2008; 99(2): 455–467, http://dx.doi.org/10.1002/bit.21572.
- Shimbara N., Atawa R., Takashina M., et al. Long-term culture of functional hepatocytes on chemically modified collagen gels. Cytotechnology 1996; 21(1): 31–43, http://dx.doi.org/10.1007/BF00364835.
- Arca H.C., Senel S. Chitosan based systems for tissue engineering Part II: soft tissues. FABAD J Pharm Sci 2008; 33: 211–226.
- Flendrig L.M., Calise F., Florio E., et al. Significantly improved survival time in pigs with complete liver ischemia treated with a novel bioartificial liver. Int J Artif Organs 1999; 22: 701–709.
- Catapano G., De Bartolo L., Vico V., Ambrosio L. Morphology and metabolism of hepatocytes cultured in Petri dishes on films and in non-woven fabrics of hyaluronic acid esters. Biomaterials 2001; 22: 659–665, http://dx.doi.org/10.1016/S0142-9612(00)00228-3.
- Gerlach J.C. Long-term liver cell cultures in bioreactors and possible application for liver support. Cell Biol Toxicol 1997; 13: 349–355.
- Mitzner S.R., Stange J., Klammt S., et al. Extracorporeal detoxification using the molecular adsorbent recirculating system for critically ill patients with liver failure. J Am Soc Nephrol 2001; 12: 75–82.
- Naruse K., Sakai Y., Nagashima J., Suzuki M., et al. Development of a new bioartificial liver module filled with porcine hepatocytes immobilized on non-woven fabric. Int J Artif Organs 1996; 6: 347–352.
- Gluck J.-M. Electrospun nanofibrous poly(ε-caprolactone) scaffolds for liver tissue engineering [dissertation]. Raleigh (NC): Carolina St. Univ.; 2007.
- Tsang V.L., Chen A.A., Cho L.M., et al. Fabrication of 3D hepatic tissues by additive photopatterning of cellular hydrogels. FASEB J 2007; 21: 790–801, http://dx.doi.org/10.1096/fj.06-7117com.
- Cho C.H., Park J., Tilles A.W., et al. Layered patterning of hepatocytes in co-culture systems using microfabricated stencils. BioTechnigues 2010; 48: 47–52, http://dx.doi.org/10.2144/000113317.
- Ryabinin V.E., Tkachev S.I., Grobovoy S.I. Ispol’zovanie efferentnykh metodov terapii i apparata «bioiskusstvennaya pechen’» pri lechenii pechenochnoy nedostatochnosti [The study of hepatic cytosolic properties and the efficiency of its use in biological liver assist device]. Vestnik RAMN — Herald of RAMS 2002; 36: 92–93.
- Powers M.J., Griffith L.G. Adhesion-guided in vitro morphogenesis in pure and mixed cell cultures. Microsc Res Tech 1998; 43: 379–384.
- Takahashi M., Sakurai M., Enosawa S., et al. Double-compartment cell culture apparatus: construction and biochemical evaluation for bioartificial liver support. Cell Transp 2006; 15: 945–952.
- Powers J.M., Domansky K., Kaazempur-Mofrad M.R., et al. A microfabricated array bioreactor for perfused 3D liver culture. Biotechnol Bioеng 2002; 78(3): 257–269; http://dx.doi.org/10.1002/bit.10143.
- Lee J.-H., Lee D.-H., Park J.-K., et al. Potentiality of immobilized pig hepatocyte spheroids in bioartificial liver system. Transplant Proc 2012; 44(4): 1012–1014, http://dx.doi.org/10.1016/j.transproceed.2012.03.010.
- Catapano G., Gerlach J.C. Bioreactors for liver tissue engineering. Topics in Tissue Engineering 2007; 3: 2–42.
- Török É., Vogel C., Lütgehetmann M., et al. Morphologycal and functional analysis of rat hepatocyte spheroids generated on poly(l-lactic acid) polymer in a pulsative flow bioreactor. Tissue Eng 2006; 12: 1881–1890, http://dx.doi.org/10.1089/ten.2006.12.1881.
- Matsumura K.N., Guevara G.R., Huston H., et al. Hybrid bioartificial liver in hepatic failure: preliminary clinical report. Surgery 1987; 101: 99–103.
- Margulis M.S., Erukhimov E.A., Andreiman L.A., Viksna L.M. Temporary organ substitution by hemoperfusion trough suspension of active donor hepatocytes in a total complex of intensive therapy in patients with acute hepatic insufficiency. Resuscitation 1989; 18: 85–94.
- Poyck P.C., Pless G., Hoekstra R., et al. In vitro comparison of two bioartificial liver systems: MELS Cell module and AMC-BAL. Int J of Artificial Organs 2007; 30(3): 183–191.
- Naka S., Takeshita K., Yamamoto T., et al. Bioartificial liver support system using porcine hepatocytes entrapped in a three-dimensional hollow fiber module with collagen gel: an evaluation in the swine acute liver failure model. Artif Organs 1999; 23: 822–828, http://dx.doi.org/10.1046/j.1525-1594.1999.06323.x.
- Iwata H., Sajiki T., Maeda Н., et al. In vitro evaluation of metabolic functions of a bioartificial liver. ASAIO J 1999; 45: 299–306.
- Migashi H., Ookawa K., Ohshima N. et al. Hepatocyte culture utilizing porous polyvinyl formal resin maintains long-term stable albumin secretion activity. J Biomaterials Sci Polymer Edition 1999; 9: 227–237.
- Parkhisenko Yu.A., Alekseev D.V. Ispol’zovanie ekstrakorporal’nykh sistem podderzhki pecheni pri ostroy ili molnienosnoy pechenochnoy nedostatochnosti v transplantologii [The use of extracorporeal liver support system in acute or fulminant hepatic failure in transplantology]. Khirurgiya. Zhurnal im. N.I. Pirogova — Surgery. Journal named after N.I. Pirogov 2004; 4: 55–60.
- Solov’ev V.V., Akatov V.S., Lezhnev E.I. Issledovanie funktsional’noy aktivnosti gepatotsitov v tkanevykh fragmentakh v novom bioreaktore «biologicheskaya iskusstvennaya pechen’» [The study of hepatocyte functional activity in tissue fragments in a novel bioreactor “biological artificial liver”]. Byulleten’ eksperimental’noy biologii i meditsiny — Bulletin of Experimental Biology and Medicine 2000; 129(6): 698–700.









