Combined Endoscopic Therapy of Sigmoid Colon Cancer Complicated by Bowel Obstruction in an Extremely Obese Patient
There has been described a case of combined endoscopic therapy (tumor pre-stenting followed by laparoscopy-assisted radical surgery) of sigmoid colon cancer complicated by bowel obstruction. A patient suffered from stage IV obesity and had undergone left nephrectomy before, which resulted in a secondary adhesive process in surgical area.
Emergency surgery of an acute neoplastic large bowel obstruction (ALBO) is connected with a high risk of complications and mortality rate (more than 30%), as well as with a high percent of conventional or temporary colostomies (up to 67%), especially in the left-sided localization of the tumor [1, 2].
In the last decades endosurgical methods of restoration of the intestinal content passage became widely used, being both a supplement and an alternative to ALBO surgical treatment. One of such methods is stenting the stenosed zone by self-expandable metal devices or stents (SEMS). In 1991 M. Dohmoto presented his first experience of using SEMS as a palliative treatment in malignant large intestine obstruction [3]. In 1994 E. Tejero et al. published their first report on the treatment of the large intestine, in which stenting was a preliminary step prior surgical intervention [4].
A.G. Fyodorov et al. [5] implanted 6 colorectal stents to 5 patients in 2010–2011. In one case bowel obstruction was of an acute character and stenting was performed as an emergency operation, in four other cases obstruction was diagnosed as a partial one.
Laparoscopic colorectal surgery originated in the early 90-s of the XX century, when Moises Jacobs in Miami, Florida, in June 1990 performed the first laparoscopically-assisted right hemicolectomy with formation of extracorporal anastomosis via minilaparotomic incision. In the same year P. Lahey made a resection of the sigmoid colon, and D. Flower — left hemicolectomy for cancer [6].
At present, laparoscopic resections in large intestine cancer are widely used in the world, though in Russia they are made much rarely because the cost of stents and equipment is rather high. Obesity of an extreme degree and previous operations are significant limiting factors in laparoscopic surgery.
Below our own observation is presented.
A patient Ch., 68 years of age, was admitted to the Surgical Unit of City Clinical Hospital No.30 on 8 September 2013 complaining of the retention of stool and gases for 3 days. He suffered from hypertension, obesity of IV degree (body mass 128 kg, height 182 cm), 12 years ago he suffered left nephrectomy for urolithiasis. On the survey radiograph of the abdominal cavity single large bowel Kloiber’s cups were determined. After spasmolytic therapy and cleansing enema patient’s condition became better, gases passed away. However, some time later the bowel inflated again. On 13 September, a survey radiograph showed multiple Kloiber’s cups again. The patient refused the suggested open operation with possible colostomy. Colonoscopy was made, which revealed stenosing tumor of the large bowel at a distance of 40 cm from the anus. As at the moment of examination stents were not available, balloon dilatation of the tumor lumen was performed, during which a portion of gases and bowel discharge moved away. Three cleansing enemas were also done.
7 hours later, when uncoated SEMS (Hanarostent, M.I. Tech, Korea) was delivered, endoscopic stenting of the tumor lumen was performed (Fig. 1). The procedure lasted 57 min. During 3 days gases were passing away, stool occurred several times. Kloiber’s cups were not determined radiographically. After the accomplishment of all needed examination procedures (US examination, histological investigation of the tumor, general clinical examination) in 12 days following stenting laparoscopically-assisted resection of the sigmoid colon with lymphodissection was performed (duration of the operation was 1 h 50 min). The length of the incision in the left iliac area amounted to 7 cm. During the operation an adhesive process was noted in the region of the lumbotomic scar, which required additional separation of adhesions.
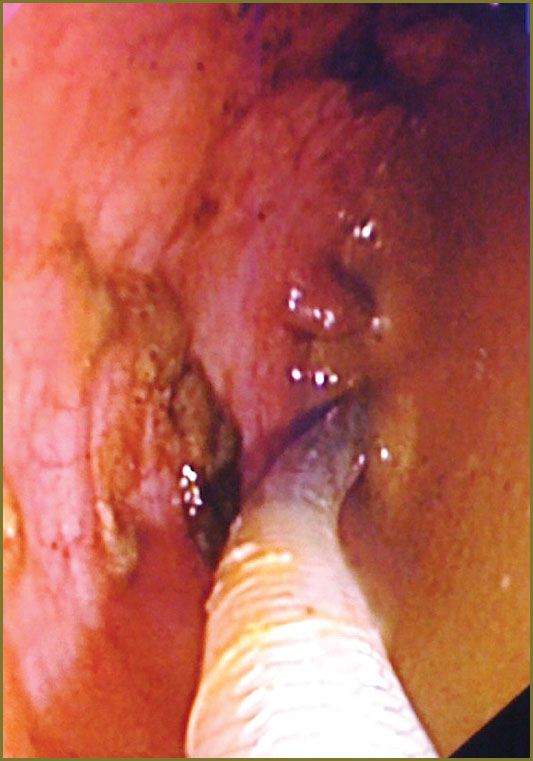 Fig. 1. A guide with a stent is introduced via the tumor lumen during colonoscopy Fig. 1. A guide with a stent is introduced via the tumor lumen during colonoscopy
|
Histological investigations of the preparation 1.10 led to the following conclusion: circular stenosing moderately-differentiated dark-cell adenocarcinoma extending to 5 cm, invading the whole wall of the colon, tumor metastasis in one lymphatic node. The line of resection is within the limits of healthy tissues (Fig. 2). Final diagnosis: “cancer of sigmoid colon T3 N1M0”.
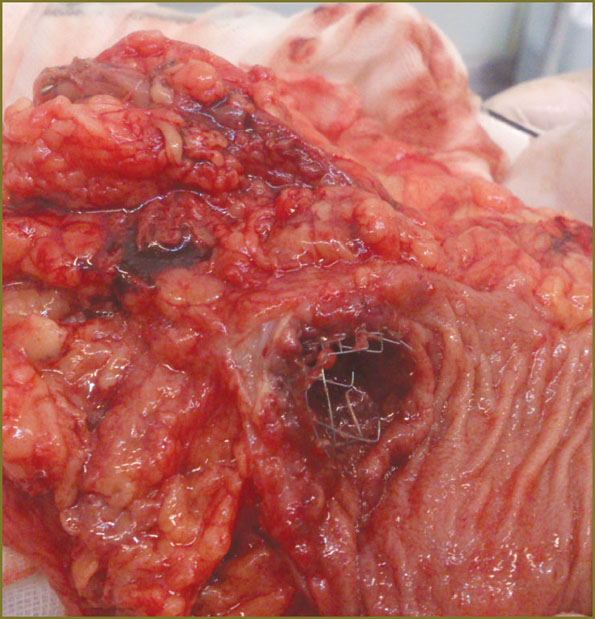 Fig. 2. Removed tumor of sigmoid colon, a stent is seen in the tumor lumen Fig. 2. Removed tumor of sigmoid colon, a stent is seen in the tumor lumen
|
The patient was discharged without complications on the 6-th day in the satisfactory condition with recommendations to be treated by polychemotherapy and other administrations made by oncologist.
Combined application of intraluminal endoscopic stenting and laparoscopically-assisted resection of the large intestine enabled us to carry on radical uneventful treatment of the patient with an extreme degree of adiposis, suffering from cancer of sigmoid colon, complicated by bowel obstruction, without ostomy construction.
References
- Hsu T.C. Comparison of one-stage resection and anastomosis of acute complete obstruction of left and right colon. Am J Surg 2005 Apr; 189(4): 384–387, http://dx.doi.org/10.1016/j.amjsurg.2004.06.046.
- Alvarez J.A., Baldonedo R.F., Bear I.G., Truan N., Pire G., Alvarez P. Presentation, treatment, and multivariate analysis of risk factors for obstructive and perforative colorectal carcinoma. Am J Surg 2005; 190(3): 376–382, http://dx.doi.org/10.1016/j.amjsurg.2005.01.045.
- Dohmoto M. New method-endoscopic implantation of rectal stent in palliative treatment of malignant stenosis. Endosc Digest 1991; 3: 1507–1512.
- Tejero E., Mainar A., Fern?ndez L., Tob?o R., De Gregorio M.A. New procedure for the treatment of the colorectal neoplastic obstructions. Dis Colon Rectum 1994; 37(11): 1158–1159.
- Fedorov A.G., Davydova S.V., Klimov A.E., Potanina O.V. Vosstanovlenie passazha soderzhimogo tolstoy kishki pri opukholevoy neprokhodimosti [Restoration of colon content passage in tumor obstruction]. Tikhookeanskiy meditsinskiy zhurnal — Pacific Medical Journal 2011; 4: 10–13.
- Jacobs M., Verdeja J.C., Goldstein H.S. Minimally invasion colon resection (laparoscopic colectomy). Surg Laparosc Endosc 1991; 1(3): 144–150.









