Optical Coherence Tomography as a Tool in Reproductive Gynecology
The objective of the investigation was to show the advisability of using optical coherence tomography (OCT) for noninvasive diagnostics and monitoring of treatments in gynecological practice for female patients of reproductive age.
Materials and Methods. OCT studies were performed during standard gynecological procedures like laparoscopy and colposcopy, as well as in course of pelvic inflammatory diseases of cervical neoplasia, with the use of an OKT1300U (BioMedTech, Russia). 330 patients of reproductive age (aged 18–45) were examined. The methods used for numeric processing of the OCT images were based on an analysis of histograms and on calculation of the first derivative of the OCT signal over depth.
Results. The use of OCT with numeric processing of the images increases the sensitivity of laparoscopy diagnosis of latent chronic salpingitis from 43.5 to 96.0%. In the case of minimal endometriosis, OCT can be used as a substitute for excisional biopsy for the visualization and verification of endometrioid heterotopias. The use of OCT in the case of cervical neoplasia in female patients of reproductive age enables a considerable decrease in surgical aggression during the diagnosis and treatment of cervical intraepithelial neoplasia and early forms of cancer.
Conclusion. The use of OCT helps to maximize individualization and organ preservation during the diagnosis and treatment of gynecological pathology, and therefore to preserve the reproductive potential of young female patients.
The reproductive function is one of the most important functions of the woman. In recent decades, issues of the preservation and restoration of reproductive health have become particularly topical. This is connected with the increase in the number of infertile couples, as well as with an increasing incidence of diseases which threaten reproductive potential.
The percentage of infertile couples in many countries constitutes about 15% and shows no sign of decreasing while 28% of these cases represent so-called unexplained infertility [1]. This high percentage of unexplained infertility is, to a great extent, connected with imperfections in the methods of diagnosis used, which are incapable of detecting the insignificant changes and latent processes which are prevalent among the reasons for reproductive dysfunction [2, 3]. As a rule, the final stage in the diagnosis of female infertility is laparoscopy. However, the relevance of this method and its possibilities are currently being disputed. Thus, as has been found, in identifying one of the most frequent causes of reproductive dysfunction, pelvic inflammatory diseases, laparoscopy demonstrates a very low sensitivity, of 27% with a high specificity of 92%, resulting in a diagnostic accuracy of 78% [4]. Nevertheless, laparoscopy remains the gold standard for clarifying the etiology of female infertility [5, 6], thus making enhancement of the procedure through the use of supplementary methods appropriate and relevant. Optical coherence tomography (OCT) is one such method and the possibilities for its complementary use with laparoscopy are currently being studied [7, 8].
A further threat to the reproductive potential of women is gynecological disease, the treatment of which may be associated with loss of reproductive function. Among the most notable diseases of this type are tumors of the female pelvic organs including malignant neoplasms. The fact that malignant tumors are getting “younger” necessitates the development of organ preservation treatment but is possible only at the early stages of the disease [9]. In its turn this determines the requirement for more effective methods of diagnosis and monitoring of the treatment: maximal information and minimal invasiveness. OCT, being a noninvasive method for obtaining information about the structure of biological tissues at the level of tissue layers, has established its value in the diagnosis of early forms of cervical neoplasia, the “youngest” oncological disease among women [10, 11]. Detection of cervical neoplasia in reproductive age women at the stage of cervical intraepithelial neoplasia (CIN) and/or cancer in situ, allows for photodynamic therapy (PDT) which is currently the least aggressive method of treatment of this pathology, enabling preservation of the reproductive function [12]. Along with its advantages, PDT has one serious disadvantage connected with impossibility of morphological control of the treatment. This determines the need for the development of effective noninvasive methods for monitoring PDT, undoubtedly including OCT, the potential of which for the evaluation of minimally invasive procedures has been demonstrated [13].
The objective of the investigation is to demonstrate the feasibility of OCT for noninvasive diagnostics and the treatment monitoring in gynecological practice among patients of reproductive age. The article presents an overview of our previous results.
Materials and Methods. In this study OCT inspection was performed to complement standard gynecological procedures like laparoscopy and colposcopy, as well as at different stages of PDT of the cervix. The instrument used was an OKT1300U (BioMedTech, Russia) with the following technical parameters: central probing wavelength of 1280 nm, in-depth resolution of 15 µm, lateral resolution of 20 µm, image acquisition rate of 8 frames per second, probing depth up to 1.4 mm. The instrument is equipped with a removable endoscopic probe 2.4 mm in diameter. The video mode allows to obtain information not only about the morphological, but also on the functional characteristics of the biotissues.
The inclusion criterion was the reproductive age of the patients, from 18 to 45. In total 330 female patients were examined with the use of OCT, including 180 patients with pathology of the pelvic organs (OCT laparoscopy) and 150 patients with early neoplasia of the cervix (OCT colposcopy), 30 of these were examined during PDT. Interpretation of the OCT images was performed in accordance with the criteria developed on the basis of morphologically verified diagnoses; the morphology data are represented in [14–15].
Methods of numeric processing of OCT images were used for objectification of the data. These were based on the analysis of histograms and the calculation of the first derivative of the OCT signal over in-depth direction [8]. The first method enables automatic differentiation of those cases which are characterized by different specific levels of OCT signal (e.g. normal tissues are characterized by a lower level of OCT signal compared to those with fibrosis), whereas the second method enables cases to be identified where contrasting areas are present in the OCT images (which is typical of edemas).
Results and Discussions
OCT in the diagnosis of infertility. We used OCT as a supplementary method during standard laparoscopy in patients with preliminary diagnoses of “unexplained infertility” with minimal clinical manifestations and non-obvious anamnesis of the disease. It was relevant that the data from the laparoscopy were also uninformative: in most cases no apparent anomalies being detected or evidence of a chronic inflammatory process or endometriosis was indirect. To obtain the OCT images an OCT probe was inserted through an extra trocar into the pelvic cavity and fixed by minimal pressing onto the serosa of the isthmic part of the fallopian tube or onto the parietal peritoneum for several seconds. The images obtained were interpreted in accordance with the previously developed criteria [15, 16].
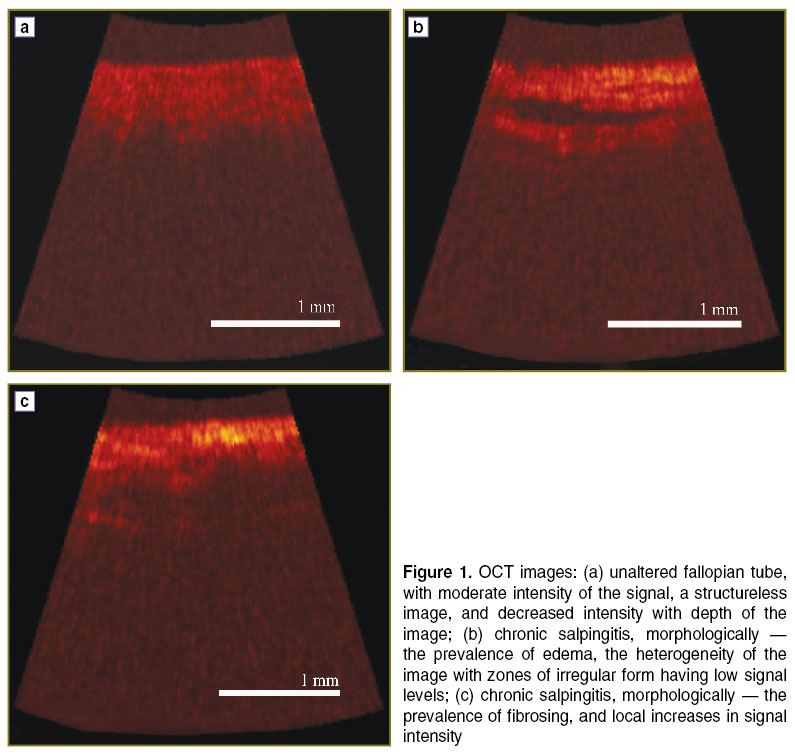
During the study, examinations of fallopian tubes revealed three completely different types of OCT image (Figure 1). A structureless image with moderate signal intensity testified to a lack of any fallopian tube pathology (Figure 1 (a)). Heterogeneity in the structure of the OCT image testified to morphological heterogeneity of the muscle layer of the fallopian tube which evidences the presence of chronic salpingitis (Figure 1 (b), (c)). It is clinically significant that the OCT images allowed us, not only to diagnose chronic salpingitis, but also to identify the pathomorphological form of the inflammation. A dominance of inclusions with a low signal level (Figure 1 (b)) testifies to a predominantly exudative pathomorphological variant, whereas the presence in the image of “bright” areas where there was a greater signal intensity testified to fibrosis processes. Frequently, OCT images with a variety of heterogeneities were encountered.
|
Figure 1. OCT images: (а) unaltered fallopian tube, with moderate intensity of the signal, a structureless image, and decreased intensity with depth of the image; (b) chronic salpingitis, morphologically — the prevalence of edema, the heterogeneity of the image with zones of irregular form having low signal levels; (c) chronic salpingitis, morphologically — the prevalence of fibrosing, and local increases in signal intensity |
The data obtained are of great clinical importance. First of all, OCT effectively increases the sensitivity of laparoscopy in regard to the recognition of chronic pelvic inflammatory diseases. We carried out an open test to identify the diagnostic accuracy of laparoscopy and OCT laparoscopy, during which the symptoms of inflammation, based on laparoscopy, and on the OCT images, were identified among 29 patients with known, morphologically proved, diagnosis of chronic salpingitis. It was found that the sensitivity of laparoscopy alone was 43.5%, whereas the complementary use of OCT increased that percentage up to 95.7%. A more accurate assessment in the diagnosis of inflammatory changes to the fallopian tubes was provided by a “blind” test where a similar result was obtained; here the sensitivity of OCT laparoscopy was 90%. A fairly good kappa index of agreement amongst specialists (0.63; confidence interval 95% [0.5082; 0.7453]) suggests the sufficient objectivity of our proposed approach [17].
Another aspect of the clinical importance of our findings relates to the possibility of the noninvasive diagnosis of pathomorphological variants of the disease. Until now, such information has been unavailable in vivo, so there has previously been no division into variants. In planning their treatment all patients underwent comprehensive therapy in accordance with the existing standards. By obtaining information regarding the prevalence of sclerosis of the muscular wall of the fallopian tube in vivo, we believe it is advisable to abandon conservative treatment in favor of assisted reproductive technologies to reduce the pill burden, the term and the cost of treatment.
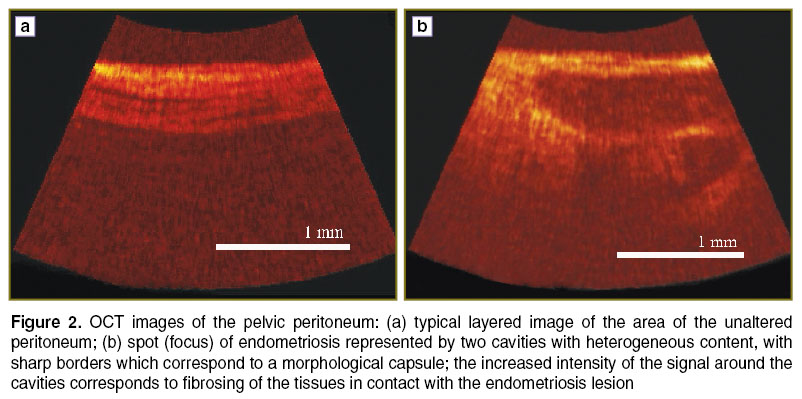
Another cause of infertility which is difficult to diagnose is the so-called minimal endometriosis. The only method of identifying this type of endometriosis is still laparoscopy, with the method of verification being histological examination of bioptates. The small size and diversity of the manifestations of endometric heterotopias, as well as the peculiarities of their localization, make their visualization, interpretation and biopsy difficult, and sometimes impossible [18]. We used OCT for probing “endometriosis-suspicious” areas of the pelvic peritoneum which had been detected during standard laparoscopy. It was found that the OCT images of unchanged peritoneum indicated that it was formed from alternating layers of thin serosa, fatty tissue, and small vessels which made up the total “laminated” image (Figure 2 (а)). In study of endometriosis, objects of irregular shape with clear contours with alternating low and high intensity signals could be visualized (Figure 2 (b)). The features of OCT images of endometriosis lesions are determined by their morphological peculiarities: the clear contours, are those bounded by the presence of a capsule, the heterogeneity of the signal — by their heterogeneous content, and the increase of the signal intensity around the inclusions — with collateral fibrosing due to the reactive perifocal inflammation. The size of the detected objects is also of importance (1–2 mm) as well as their localization at arbitrary depth with regard to the peritoneum surface. These changes are hard to identify in standard laparoscopy.
|
Figure 2. OCT images of the pelvic peritoneum: (а) typical layered image of the area of the unaltered peritoneum; (b) spot (focus) of endometriosis represented by two cavities with heterogeneous content, with sharp borders which correspond to a morphological capsule; the increased intensity of the signal around the cavities corresponds to fibrosing of the tissues in contact with the endometriosis lesion |
The example provided shows that the capacity of OCT to visualize the inner structure of the tissue can be successfully used for the detection of minimal endometriosis. In the case of complicated localization of endometriosis heterotopias around the vessels, on the visceral peritoneum of the fallopian tube, or in the gate area of the ovary, biopsy is difficult. In these cases, OCT can substitute such an invasive procedure.
OCT in the diagnostics of cervical neoplasia. The wider use of noninvasive diagnostic technologies in the group of patients of reproductive age is reasonable, not only for diagnosis of infertility, but also for other gynecological pathology, such as cervical neoplasia. Firstly, cervical cancer is “the youngest” among all female tumors. Early revealing CIN and cancer in situ makes it possible to preserve fertility, but there is a problem of the effective diagnosis of the pathology of the cervix [19]. This is connected not only with the insufficient sensitivity of traditional methods of diagnosis but also with the low specificity of the gold standard — colposcopy. To compensate for this, the use of multi-focus biopsy or wide excisions of the cervix have been suggested. This diagnostic aggression is, to a certain degree, a risk to reproductive potential.
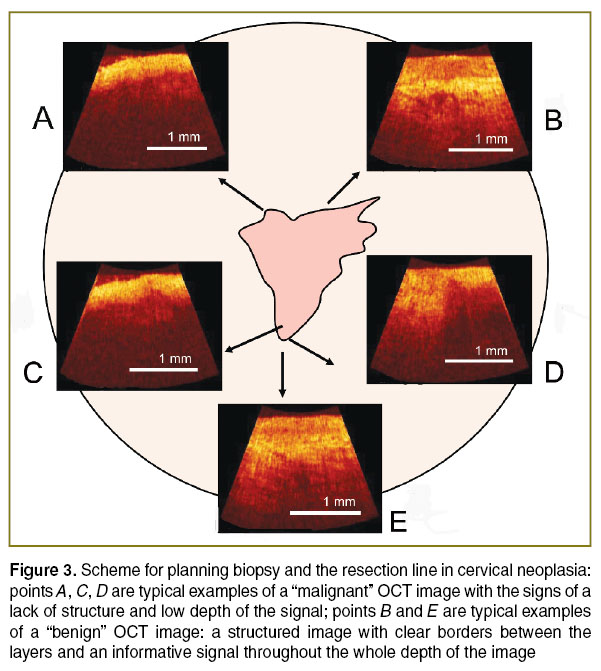
In this work we have suggested the use of OCT to reduce the number of unwarranted excision procedures. First and foremost, the OCT criteria which have been developed in relation to neoplasia of the cervix [10, 14] allow us confidently to abandon the need for biopsy after obtaining a typical “benign” OCT image (points B and E in Figure 3) even if there are so-called atypical colposcopic signs. However, if there are OCT signs of malignancy (points А, C and D in Figure 3) biopsy is obligatory. This approach can reduce the number of false-positive conclusions from colposcopy, and in about 40% of cases allows us to refuse from biopsy [20]. Long-term observation of patients (for more than 3 years) have not revealed any progression of the pathology of the cervix in those cases of refusal from invasive diagnostics, and this retrospectively confirms the adequacy of the applied OCT criteria, and such tactics in general.
|
Figure 3. Scheme for planning biopsy and the resection line in cervical neoplasia: points A, C, D are typical examples of a “malignant” OCT image with the signs of a lack of structure and low depth of the signal; points B and E are typical examples of a “benign” OCT image: a structured image with clear borders between the layers and an informative signal throughout the whole depth of the image |
Optimization of the algorithm for the diagnosis of neoplasia of the cervix with the use of OCT is not only relevant to biopsy of the cervix. The presence of “malignant” signs in OCT images in different sectors of the cervix is a justified indication for diagnostic excision rather local spot biopsy. When planning the resection line it is also advisable to use OCT. In Figure 3 (point D) it can be seen that in an OCT investigation of the visual border of the pathological zone the image shows the transition of one type of structure into another, and only after retreating several millimeters it is possible to obtain a typical “benign” image. This information can be used during excision to ensure the adequate removal of the tumor. This approach allows us to provide maximal oncological effectiveness for the resection whilst retaining functional preservation of the organs.
In recent years photodynamic therapy has been implemented as a standard for treating patients of childbearing age with early neoplasia of the cervix, as an alternative to using surgical methods.
Along with a number of advantages, PDT has some limitations: the unpredictability of the photodynamic reactions, the influence of the degree of tumor oxygenation on the results, the lack of excision material for morphological monitoring of the treatment and the empirical character of the mode selection [21]. It is possible to minimize the influence of the weaknesses of PDT with the use of effective methods of monitoring (which are noninvasive and realized quickly in real-time) and here OCT undoubtedly has the required characteristics.
Figure 4 shows a sequence of OCT images of the cervix of female patient M., 32 years old, with a diagnosis of CIN III. Before the treatment, the OCT criteria (structureless and with reduced signal depth) correspond to the diagnosis (Figure 4 (а)). Two hours after the injection of photosensitizer, and directly after the laser exposure the OCT image demonstrates signs of structural change occurred manifested by the increased contrast in the image indicating the typical pathomorphological reaction, tissue edema. (Figure 4 (b)). After one day (Figure 4 (c)) signs of hyperemia and blood stasis are increasing, while, after 6 days (Figure 4 (d)), signs of total tumor necrosis are present due to total failure of the blood circulation. After a month (Figure 4 (e)) no tumor was registered in the control biopsy, and there were the signs of repair associated with reactive inflammatory changes.
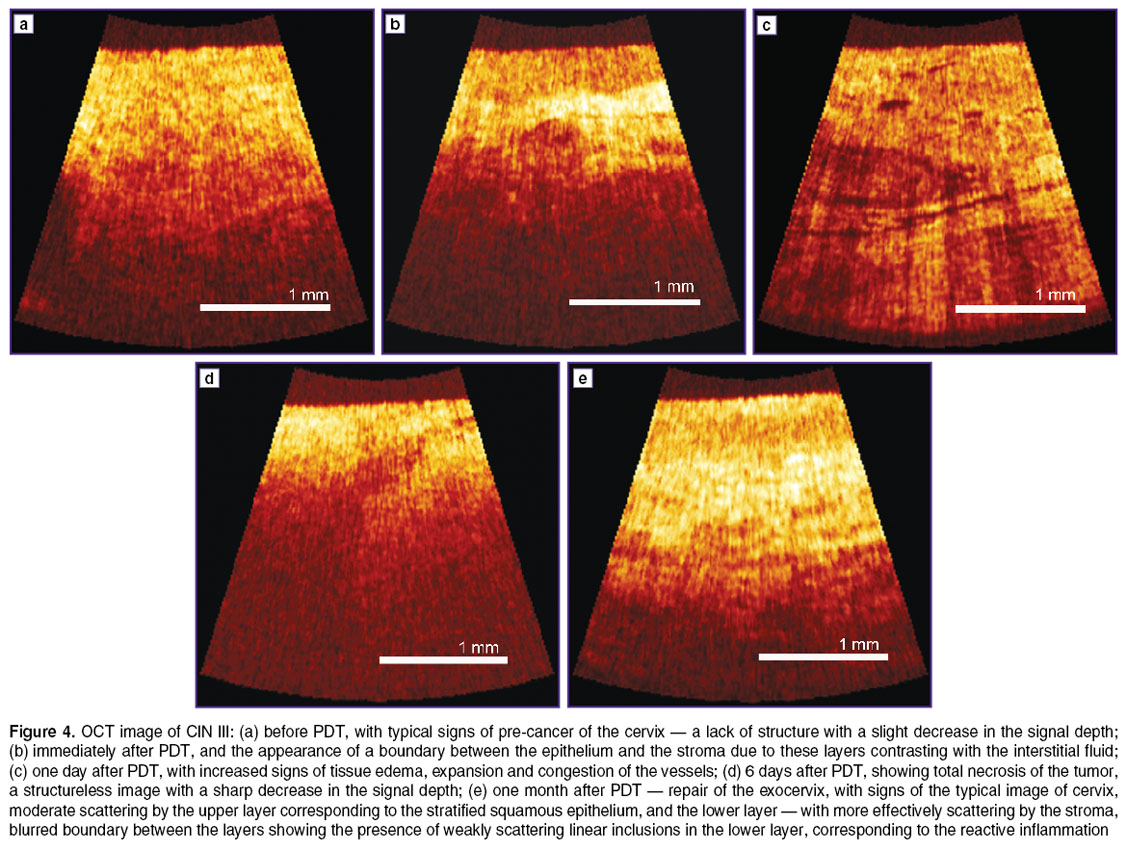
The example provided vividly indicates the possibility for noninvasive observation of the structural changes of the ectocervix in response to PDT; and it demonstrates the prospects of OCT for the dynamic monitoring of complete and timely pathomorphological reactions.
It should be said that the mechanism of PDT is based on the interaction of several components (the photosensitizer, light and oxygen) with the implementation of several types of reaction [21]. Unfortunately, OCT can only retrospectively assess the results of PDT, but not the process of action in real time. This is why, for effective monitoring, it is useful to combine several methods of bioimaging. In our view its combination with fluorescent visualization is particularly effective, as it allows assessment of the accumulation andphotobleaching of the photosensitizer [22]. Other authors have also suggested combinations of methods, for example, for the assessment of photosensitizer photobleaching and the dynamics of singlet oxygen [23]. Another approach is based on observation of the basic PDT mechanism with an assessment of microcirculation and tissue oxygenation [24]. In this regard a modification of the OCT approach with implementation of the visualization of the microvasculature is required [25].
However, despite we have shown the attractiveness of OCT in situations where its noninvasiveness is indispensable, there is a need for further enhancement and modification of the method. One such is automation of the interpretation of the OCT images. It should be noted that a specialist’s subjective assessment of a diagnostic image can sometimes differ from the actual situation due either to the changes in the OCT image not being readily visible or to insufficient training of the specialist. In these cases it would be effective to apply numeric processing to the OCT images as this could numerically characterize the image to help avoid subjectivity in the assessment. For differential diagnostics it is logical to use several numeric criteria that reveal different changes in the object and which therefore allow not only identification of the presence of particular pathologies, but could also determine their extent. In the OCT investigations of fallopian tubes we used an approach involving the calculation of the two values from OCT images which characterize the degree of edema and tissue fibrosing. The use of these values in the assessment of diagnostic OCT images should enable increased sensitivity of the method up to 96% compared to the 90% already demonstrated in “blind” testing without numeric processing [8, 17].
Conclusion. Our study showed that employment of OCT as a supplementary tool during standard procedures increases the effectiveness of the diagnosis of those gynecological pathological states which are difficult to recognize. The use of OCT for patients of reproductive age is justified to a great extent as, in this case, the enhanced information is not accompanied by any additional invasiveness.
As a supplementary method for recognition of the causes of infertility OCT has shown a high sensitivity to latent forms of pelvic inflammatory diseases. The possibility of visualizing and verifying minimal endometriosis with OCT is of great interest.
The complementary use of OCT during colposcopy allows a reduction in the aggressiveness of the diagnosis of pre-cancer and early forms of cervical cancer. OCT monitoring of photodynamic therapy contributes to the optimization of this organ-preserving method of treatment of early forms of cervical neoplasia.
One further advantage is provided by the numeric processing of OCT images as it will allow us to avoid the subjectivity of specialists during the assessment of images and will therefore increase the diagnostic accuracy of the method.
And finally the use of OCT can contribute to the maximal individualization and organ preservation during the diagnosis and treatment of gynecological pathology, and therefore to the preservation of the reproductive potential of female patients of reproductive age.
Study Funding. This article is a review of our studies which were, in different years, financed by the Program of the Presidium of the Russian Academy of Sciences “Fundamental Sciences to Medicine”, partially by grants from the Russian Foundation for Basic Research and those linked to the projects of the Ministry of Education and Sciences of the Russian Federation, including the studies currently being performed on PDT monitoring, where the clinical trials are supported by Project No.14.В25.31.0015, technological studies on Project RFMEFI60414X0027.
Conflicts of Interest. The authors have no conflicts of interest.
References
- Kamath M.S., Bhattacharya S. Demographics of infertility and management of unexplained infertility. Best Pract Res Clin Obstet Gynaecol 2012 Dec; 26(6): 729–738,http://dx.doi.org/10.1016/j.bpobgyn.2012.08.001.
- Gleicher N., Barad D. Unexplained infertility: does it really exist? Hum Reprod 2006 Aug; 21(8): 1951–1955, http://dx.doi.org/10.1093/humrep/del135.
- Siristatidis C., Bhattacharya S. Unexplained infertility: does it really exist? Does it matter? Hum Reprod 2007 Aug; 22(8): 2084–2087, http://dx.doi.org/10.1093/humrep/dem117.
- Molander P., Finne P., Sjöberg J., Sellors J., Paavonen J. Observer agreement with laparoscopic diagnosis of pelvic inflammatory disease using photographs. Obstet Gynecol 2003; 101(5 Pt 1): 875–880, http://dx.doi.org/10.1016/s0029-7844(03)00013-9.
- Tsuji I., Ami K., Miyazaki A., Hujinami N., Hoshiai H. Benefit of diagnostic laparoscopy for patients with unexplained infertility and normal hysterosalpingography findings. Tohoku J Exp Med 2009 Sep; 219(1): 39–42, http://dx.doi.org/10.1620/tjem.219.39.
- Merviel P., Lourdel E., Brzakowski M., Garriot B., Mamy L., Gagneur O., Nasreddine A. Should a laparoscopy be necessary in case of infertility with normal tubes at hysterosalpingography? Gynecol Obstet Fertil 2011 Sep; 39(9): 504–508, http://dx.doi.org/10.1016/j.gyobfe.2011.07.008.
- Ascencio M., Collinet P., Cosson M., Mordon S. The role and value of optical coherence tomography in gynecology. J Gynecol Obstet Biol Reprod (Paris) 2007 Dec; 36(8): 749–755,http://dx.doi.org/10.1016/j.jgyn.2007.07.005.
- Kirillin М., Panteleeva O., Yunusova E., Donchenko E., Shakhova N. Criteria for pathology recognition in OCT of fallopian tubes. J Biomed Opt 2012 Aug; 17(8): 1411–1415,http://dx.doi.org/10.1117/1.JBO.17.8.081413.
- Eskander R.N., Randall L.M., Berman M.L., Tewari K.S., Disaia P.J., Bristow R.E. Fertility preserving options in patients with gynecologic malignancies. Am J Obstet Gynecol 2011 Aug; 205(2): 103–110, http://dx.doi.org/10.1016/j.ajog.2011.01.025.
- Kuznetsova I.A., Shakhova N.M., Kachalina T.S., Yunusova E.E., Kiseleva E.B., Karabut M.M. Specific features of colposcopic evidence during optical coherence tomography. Akusherstvo i ginekologiya 2011; 5: 64–67.
- Gallwas J.K., Turk L., Stepp H., Mueller S., Ochsenkuehn R., Friese K., Dannecker C. Optical coherence tomography for the diagnosis of cervical intraepithelial neoplasia. Lasers Surg Med 2011 Mar; 43(3): 206–212, http://dx.doi.org/10.1002/lsm.21030.
- Soergel P, Hillemanns P. Photodynamic therapy for intraepithelial neoplasia of the lower genital tract. Photodiagnosis Photodyn Ther 2010 Mar; 7(1): 10–14, http://dx.doi.org/10.1016/j.pdpdt.2009.12.007.
- Li Z., Shen J.H., Kozub J.A., Prasad R., Lu P., Joos K.M. Miniature forward-imaging B-scan optical coherence tomography probe to guide real-time laser ablation. Lasers Surg Med 2014 Mar; 46(3): 193–202, http://dx.doi.org/10.1002/lsm.22214.
- Kuznetsova I.A., Gladkova N.D., Gelikonov V.M., Belinson J.L., Shakhova N.M., Feldchtein F.I. OCT in gynecology. In: Optical coherence tomography: technology and applications. Ed. by Drexler W., Fujimoto J.G. Springer Berlin Heidelberg; 2008; p. 1211–1240, http://dx.doi.org/10.1007/978-3-540-77550-8_39.
- Panteleeva O.G., Shakhov B.E., Yunusova K.E., Kirillin M.Yu., Shakhova N.M. Optical introscopy is a new diagnostic technique in reproductive medicine. Vestnik rentgenologii i radiologii 2012; 4: 50–55.
- Panteleeva O.G., Shakhova N.M., Monakhov A.G. OCT laparoscopy in the diagnosis of “minor forms” of endometriosis. Sovremennye tehnologii v medicine 2011; 2: 92–95.
- Panteleeva O.G., Zinov’ev A.N., Yunusova K.E., Kirillin M.Yu., Shakhova N.M. Diagnostic possibilities of optical introscopy in revealing the causes of impaired reproductive health in women. Rossiyskiy vestnik akushera-ginekologa 2013; 5: 53–57.
- Chamié L.P., Blasbalg R., Pereira R.M.A., Warmbrand G., Serafini P.C. Findings of pelvic endometriosis at transvaginal US, MR imaging, and laparoscopy. Radiographics 2011 Jul–Aug; 31(4): E77–Е100, http://dx.doi.org/10.1148/rg.314105193.
- Rogovskaia S.I., Badalova L.A. Evaluation of the clinical and economic efficiency of diagnostic methods for cervical neoplasias. Rossiyskiy vestnik akushera-ginekologa 2011; 4: 39–43.
- Shakhova N., Kuznetsova I., Yunusova K., Kiseleva E. Diagnosis of neoplastic processes in the uterine cervix. Part 2. Photonics for health care. In: Handbook of biophotonics. Ed. by Popp J., Tuchin V.V., Chiou A., Heinemann S. Wiley-VCH; 2012; p. 877–884, http://dx.doi.org/10.1002/9783527643981.bphot065.
- Agostinis P., Berg K., Cengel K.A., Foster T.H., Girotti A.W., Gollnick S.O., Hahn S.M., Hamblin M.R., Juzeniene A., Kessel D., Korbelik M., Moan J., Mroz P., Nowis D., Piette J., Wilson B.C., Golab J. Photodynamic therapy of cancer: an update. CA Cancer J Clin 2011 Jul–Aug; 61(4): 250–281, http://dx.doi.org/10.3322/caac.20114.
- Wang Y., Gu Y., Liao X., Chen R., Ding H. Fluorescence monitoring of a photosensitizer and prediction of the therapeutic effect of photodynamic therapy for port wine stains. Exp Biol Med 2010 Feb; 235(2): 175–180, http://dx.doi.org/10.1258/ebm.2009.009294.
- Jarvi M.T., Patterson M.S., Wilson B.C. Insights into photodynamic therapy dosimetry: simultaneous singlet oxygen luminescence and photosensitizer photobleaching measurements. Biophys J 2012 Feb; 102(3): 661–671, http://dx.doi.org/10.1016/j.bpj.2011.12.043.
- Tyrrell J., Thorn C., Shore A., Campbell S., Curnow A. Oxygen saturation and perfusion changes during dermatological methylaminolaevulinate photodynamic therapy. Br J Dermatol 2011 Dec; 165(6): 1323–1331, http://dx.doi.org/10.1111/j.1365-2133.2011.10554.x.
- Mariampillai A., Leung M.K., Jarvi M., Standish B.A., Lee K., Wilson B.C., Vitkin A., Yang V.X.D. Optimized speckle variance OCT imaging of microvasculature. Opt Lett 2010 Apr; 35(8): 1257–1259, http://dx.doi.org/10.1364/OL.35.001257.









