Assessment of Chronic Subdural Hematoma Perifocal Zone Microvasculature According to Perfusion Computerized Tomography Data
The aim of the investigation was to explore possibilities of assessment of cerebral microcirculation and blood flow autoregulation in chronic subdural hematoma (CSH) perifocal zone using present-day algorithms of perfusion computerized tomography.
Materials and Methods. The concentric retrospective non-randomized study comprised 20 patients with unilateral CSH developed in result of craniocerebral injury sustained at term from 15 days to several months to admission date. Mean age of the casualties was 54.7±15.6 years (from 17 to 87 years old). 11 patients had the CSH settled on the right, while 9 patients had the CSH settled on the left. Average hematoma volume amounted to 84.2±12.4 cm3 (from 56 to 117 cm3), condition severity according to Markwalder scale was 1.8±0.5 points (from 0 to 3 points).
Colored perfusion parameter charts were plotted to describe cerebral perfusion in the cortex area adjacent to CSH and in the symmetrical area of the opposite hemisphere without the use and with the use of the mode (algorithm) for perfusion computation exclusive of flows in Remote Vessels great vessels.
Results. Perfusion indices of microvasculature in the CSH perifocal zone have no statistically significant variations from the norm and indices in the symmetrical area of the opposite hemisphere. This statement holds for assessment of perfusion status both without the use and with the use of perfusion calculation algorithm exclusive of flows in great vessels.
Conclusion. Constancy of microvasculature perfusion in the CSH perifocal zone is indicative of cerebral blood flow autoregulation retention in patients with chronic subdural hematomas.
Use of present-day cerebral perfusion assessment algorithms allows for CSH forecast in casualties with craniocerebral injury. Development of cerebral hyperperfusion local nidi, which do not affect the pial flow in patients who had a cerebral damage may serve as an early marker of CSH capsule formation with cerebral compression development.
The chronic subdural hematoma (CSH) is a disease characterized by formation of capsule around the subdural hemorrhage, which causes local and general cerebral compression. Typically, CSHs are formed after craniocerebral injury [1].
One of the key factors determining the clinical course and outcome in such patients are reactions of microvasculature in CSH-adjacent area of cerebral cortex named as perihematoma [2, 3] or perifocal [4].
It is thought [1] that just cerebral circulation disturbances and blood flow autoregulation peculiarities in this zone cause neurologic impairmentbefore operation and development of complications in the early postoperative period in case of CSH: cerebrum collapse, hematoma backset, tension pneumocephalus and secondary hemorrhages.
Information about status of cerebral microcirculation and autoregulation in this zone is still conflicting [2–5]. One of the reasons for such conflicts is inadequacy of software algorithms used for computation of cerebral perfusion indicators in computerized tomography [6–8]. Development of computer-tomography algorithms for perfusion parameter computation without the data on blood flow in cerebrum great vessels allowed for assessment of specifically pial blood flow nature in the “zone of interest” [8–10]. One of such algorithms is Remote Vessels on Philips Ingenuity CT tomograph (Philips Medical Systems, USA). Their use allowed for considerable increase of cerebral blood flow status vision and ascertain mechanism, which support microcirculation, inclusive of the CSH perifocal zone, and thereupon assess cerebral blood flow autoregulation status in patients with CSH.
The aim of the investigation was to explore possibilities of assessment of cerebral microcirculation and blood flow autoregulation in chronic subdural hematoma perifocal zone using present-day algorithms of perfusion computerized tomography.
Materials and Methods. The concentric retrospective non-randomized study comprised 20 patients (12 men and 8 women) with unilateral CSH who received medical treatment in the Nizhny Novgorod Regional Traumatology Center of N.A. Semashko Nizhny Novgorod Regional Clinical Hospital from January 2013 to March 2014. The reason for CSH development was craniocerebral injury sustained at term from 15 days to several months to admission date. Mean age of the casualties was 54.7±15.6 years (from 17 to 87 years old). The wakefulness level according to the Glasgow coma scale before the study was on the average 13.1±0.5 points (from 11 to 15 points). 11 patients had the CSH settled on the right, while 9 patients had the CSH settled on the left. Average hematoma volume calculated by the known ovoid [1] volume formula amounted to 84.2±12.4 cm3 (from 56 to 117 cm3). All hematomas had hypodense characteristics during CT examination. Average midline shift at pellucid septum level was 7.1±1.4 mm (from 5 to 12 mm) on the average. The condition severity was assessed according to Markwalder scale [11] and amounted to 1.8±0.5 points (from 0 to 3 points) on the average.
Our sampling did not include patients with CSH in decompensated condition (severity according to Markwalder: 4 points) and ambilateral hematomas.
This retrospective study was approved by the Ethics Committee of the Nizhny Novgorod State Medical Academy and meets Declaration of Helsinki requirements (adopted in June 1964 (Helsinki, Finland) and revised in October 2000 (Edinburgh, Scotland)). All patients gave written informed consent for scientific analysis of their data.
All patients were operated on the first day after the perfusion study. All patients were operated under general anesthesia with application of a single hole in temporoparietal area on CSH side, perforation and draining the hematoma cavity using the tube drainage to the external sterile system Pleurofix (B. Braun Melsungen AG, Germany). The drainage was carried out for 48 h, upon which the drainage was removed. There were no fatalities in the study group.
Upon drainage completion, in all patients, they noted pneumocephalus and residual hematomas, which volume did not exceed 30% of the initial volume. There were neither secondary hemorrhages nor cerebrum collapse.
Cerebral microcirculation was studies using the cerebrum perfusion computerized tomography (PCT) method. The PCT was carried out on 64-slice tomograph Philips Ingenuity CT (Philips Medical Systems, USA) during the first day from the moment of patients admission to the hospital before surgical interference.
The record of perfusion study [12] comprised initial un-enhanced brain imaging. 32 mm thick scanned area was set parallel to the plane of CSH maximum thickness.
Then we carried out 8 extended scans of this area for 55 seconds against contrast medium infusion (Brain Perfusion mode). The contrast medium (Ultravist 370; Shering AG, Germany) was infused by automatic injector (Visitron CT, Medrad, USA) to the cubital vein via a standard catheter at the rate of 5 ml/s for 8 s per 1 study.
The scan data were transferred to a workstation and analyzed in a standard program Philips Ingenuity Core (Philips Heathcare Nederland BV, the Netherlands, 2013, v.3.5.5.25007). Arterial and venous vessel definition markers were set according to the recommendations [12]: in А2 views of anterior cerebral artery segment and posterior third of the superior sagittal sinus, respectively.
From then on, perfusion parameter charts were plotted to describe the cerebral perfusion: cerebral blood flow (CBF), cerebral blood volume (CBV), mean time transit (MTT), time to peak (TTP).
After that they turned on Remote Vessels mode whereby automatically excluded voxels from computation, which reflected blood flows in great vessels, and plotted refined perfusion charts of the same parameters in the same patients.
According to recommendations [12], normal parameter values were considered to be: CBF — 48.8±10.1 ml/100 g·min; CBV — 3.3±0.6 ml/100 g; MTT — 4.3±0.8 s.
The specified parameters in all patients were assessed quantitatively simultaneously in the cortex area adjacent to CSH and in the symmetrical area of the opposite hemisphere without the use and with the use of Remote Vessels mode (See the Figure).
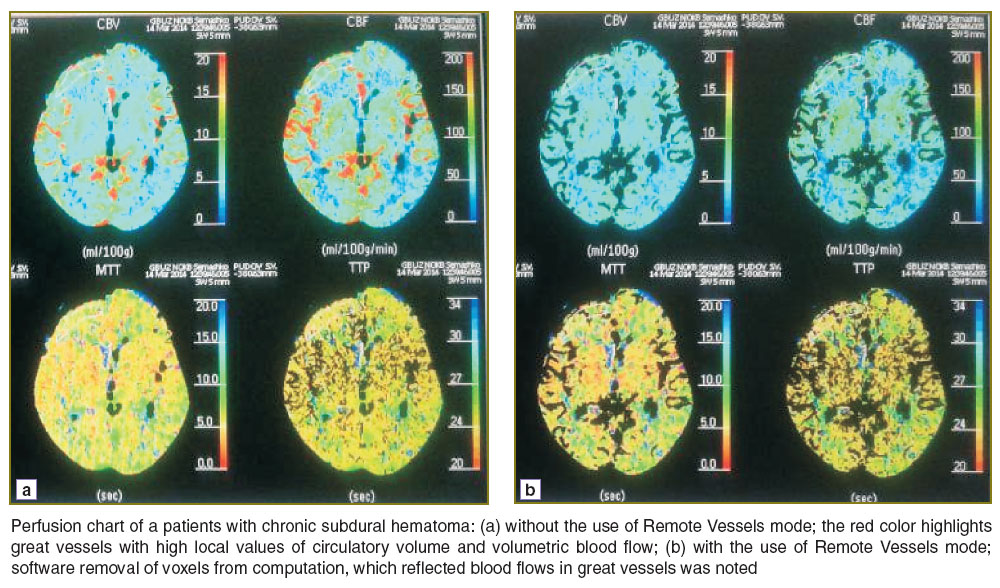 |
Perfusion chart of a patients with chronic subdural hematoma: (а) without the use of Remote Vessels mode; the red color highlights great vessels with high local values of circulatory volume and volumetric blood flow; (b) with the use of Remote Vessels mode; software removal of voxels from computation, which reflected blood flows in great vessels was noted |
PCT results obtained without the use of Remote Vessels mode made up group 1 of considered data, and the results obtained with the use of this mode in the same patients and in the same areas/zones for the same period of time made up group 2.
The data was normally distributed thus were presented in form of the average ± root mean square deviation (M±σ). Comparison between the groups was drawn according to t-Student criteria. Correlation analysis was carried out with computation of Spearman correlation coefficient. The level of significance was taken as p<0.01. Statistica 7.0 (StatSoft Inc., USA, 2004) software was used for analysis performance.
Results. Comparison with normal perfusion indicator values in CSH perifocal zone when using computation algorithm, which includes computation of flows in great vessels (group 1) showed statistically significant (p<0.01) increase of CBV and CBF and no statistically significant increase of МТТ and ТТР (See the Table). At the same time, after use of Remote Vessels PCT mode (group 2) there were no reliable change of perfusion parameters in the perifocal zone as compared to the normal value.
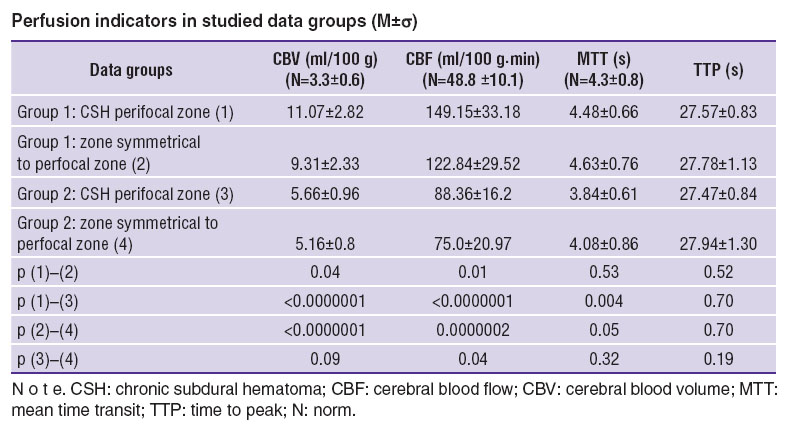 Perfusion indicators in studied data groups (M±σ) Perfusion indicators in studied data groups (M±σ)
|
In much the same way, by comparison with normal perfusion indicators in the undamaged hemi sphere zone calculated without the use of Remote Vessels mode, there was found a statistically significant increase of CBV and CBF (p<0.01) and no significant changes of MTT and TTP. When using the mode, parameters of microcirculation in the undamaged hemi sphere zone had no statistically significant differences from normal values.
Comparison of cerebral perfusion indicators in CSH perifocal zone and symmetrical area of the opposite hemi sphere without the use of refining algorithms showed statistically significant increase of volumetric blood flow in the perifocal zone (p=0.01). Other indicators had no significant changes.
However, the use of Remote Vessels refining algorithm showed no straight changes of microvasculature perfusion indicators neither on the hematoma side nor on the opposite side.
Correlation analysis showed no statistically significant dependence between indicators of perfusion, CSH volume and severity according to Markwalder scale.
Discussion. One of the fundamental properties of cerebral blood flow is its ability to support constancy of microvasculature perfusion under conditions of arterial and intra-cranial pressure variation [13]. This property is call cerebral autoregulation [14] in the modern literature. It was noted that cerebral perfusion indicators and autoregulation condition are strongly interrelated [13], and disturbances of microvasculature perfusion result from damage of autoregulation mechanisms [15, 16].
Up to the present day it was thought that in case of CSH, cerebral blood flow autoregulation mechanisms are damaged it shows itself by disturbances of cerebral microcirculation with development of hyperemia and hyperperfusion syndromes. Thus, the paper of Slotty et al. [3] demonstrates statistically significant increase of CBV and CBF in case of CSH as compared to symmetrical zones of the opposite hemi sphere, and time characteristics (MTT and TTP) did not change significantly what corresponds to hyperemia and hyperperfusion [15–18] patterns and according to the authors’ opinion are indicative of cerebral autoregulation disturbance. However, such conclusions as well as the fact that examinations were carried out on 16-slice tomograph without the use of Remote Vessels refining algorithms served as the basis for critical comments [2] on the paper of Slotty et al. [3].
Our study made use of 64-slice tomograph PCT with the algorithm, which excluded great vessels blood flows from the computation, which allowed for adequate assessment of perfusion exactly in the pial flow of CSH perifocal zone. In result, it was found that microvasculature perfusion indicators of the zone adjacent to CSH have no statistically significant differences from such indicators of the opposite hemi sphere symmetrical zone.
The obtained data quite probably is evidence of constancy of microvasculature perfusion in the CSH perifocal zone and, consequently, retention of cerebral blood flow autoregulation in patients with this pathology, which ties up with the work [19].
We are of the opinion that hyperemia and hyperperfusion in CSH perifocal zone, described in prior studies [2, 3], does not affect the cerebral microvasculature since no pial perfusion disturbances were found.
The reason for development of these syndromes in the CSH perifocal zone can be formation of de novo vessels in the capsule with development of super-capillary shunting phenomena leading to increase of volumetric blood flow [20]. In this regard, the results, which we have obtained provide strong evidence of the fact that development of cerebral hyperperfusion local nidi, which do not affect the pial flow in patients who had a cerebral damage may serve as an early marker of CSH capsule formation with cerebral compression development. This fact can provide the basis for the system of early CSH and cerebral compression development detection according to discovery of cerebral perfusion specific characteristics.
It is necessary to point out that such a study has a number of methodological limitations, the main one of which consists in impossibility of dynamic non-invasive assessment of perihematoma perfusion condition without repeated PCT scanning.
Moreover, perifocal zone perfusion assessment peculiarities need to be studied in patients with ambilateral CSHs as well as in patients with CSH in decompensated condition.
Conclusion. Perfusion indices of microvasculature in the perifocal zone of chronic subdural hematoma have no statistically significant variations from the indices in the symmetrical area of the opposite hemisphere. Constancy of microvasculature perfusion is indicative of cerebral blood flow autoregulation retention in patients with chronic subdural hematomas.
Study Funding and Conflicts of Interest. This study was not supported by any financial sources, and there is no conflicts of interest associated with the research.
References
- Konovalov A.N., Potapov A.A., Likhterman L.B., et al. Rekonstruktivnaya i minimal'no invazivnaya khirurgiya posledstviy cherepno-mozgovoy travmy [Reconstructive and minimally invasive surgery of craniocerebral injury consequences]. Moscow: Novoe vremya; 2013; 320 p.
- Aries M.J., Budohoski K.P., Metting Z., van der Naalt J. Cerebral perfusion changes in chronic subdural hematoma. J Neurotrauma 2013; 30(19): 1680, http://dx.doi.org/10.1089/neu.2013.2876.
- Slotty P.J., Kamp M.A., Steiger S.H.-J., Cornelius J.F., Macht S., Stummer W., Turowski B. Cerebral perfusion in chronic subdural hematoma. J Neurotrauma 2012; 30(5): 347–351, http://dx.doi.org/10.1089/neu.2012.2644.
- Tanaka A., Kimura M., Yoshinaga S., Ohkawa M. Computed tomography and cerebral blood flow correlations of mental changes in chronic subdural hematoma. Neurosurgery 1992; 30(3): 370–377, http://dx.doi.org/10.1227/00006123-199203000-00010.
- Okuyama T., Saito K., Fukuyama K., Yamamoto K., Morimoto M., Aburano T. Clinical study of cerebral blood flow in unilateral chronic subdural hematoma measured by 99mTc-HMPAO SPECT. No To Shinkei 2000; 52(2): 141–147.
- Tang J., Ai J., Macdonald R.L. Developing a model of chronic subdural hematoma. Acta Neurochir Suppl 2011; 111: 25–29, http://dx.doi.org/10.1007/978-3-7091-0693-8_5.
- Salvant J.B. Jr., Muizelaar J.P. Changes in cerebral blood flow and metabolism related to the presence of subdural hematoma. Neurosurgery 1993; 33(3): 387–393, http://dx.doi.org/10.1227/00006123-199309000-00006.
- Abels B., Villablanca J.P., Tomandl B.F., Uder M., Lell M.M. Acute stroke: a comparison of different CT perfusion algorithms and validation of ischaemic lesions by follow-up imaging. Eur Radiol 2012; 22(12): 2559–2567, http://dx.doi.org/10.1007/s00330-012-2529-8.
- Campbell B.C., Christensen S., Levi C.R., Desmond P.M., Donnan G.A., Davis S.M., Parsons M.W. Cerebral blood flow is the optimal CT perfusion parameter for assessing infarct core. Stroke 2011; 42(12): 3435–3440, http://dx.doi.org/10.1161/STROKEAHA.111.618355.
- Kate M.P., Hansen M.B., Mouridsen K., Østergaard L., Choi V., Gould B.E., McCourt R., Hill M.D., Demchuk A.M., Coutts S.B., Dowlatshahi D., Emery D.J., Buck B.H., Butcher K.S.; ICHADAPT Investigators. Blood pressure reduction does not reduce perihematoma oxygenation: a CT perfusion study. J Cereb Blood Flow Metab 2014; 34(1): 81–86, http://dx.doi.org/10.1038/jcbfm.2013.164.
- Markwalder T.M. Chronic subdural hematomas: a review. J Neurosurg 1981; 54(5): 637–645, http://dx.doi.org/10.3171/jns.1981.54.5.0637.
- Zakharova N.E., Potapov A.A., Kornienko V.N., Pronin I.N., Zaytsev O.S., Gavrilov A.G., Kravchuk A.D., Oshorov A.V., Sychev A.A., Alexandrova E.V., Fadeeva L.M., Takush S.V., Polupan A.A. Peculiarities of regional cerebral blood flow, intracranial pressure and cerebral perfusion pressure parameters in severe brain trauma. Luchevaya diagnostika i terapiya 2012; 3: 79–91.
- Varsos G.V., de Riva N., Smielewski P., Pickard J.D., Brady K.M., Reinhard M., Avolio A., Czosnyka M. Critical closing pressure during intracranial pressure plateau waves. Neurocrit Care 2013; 18(3): 341–348, http://dx.doi.org/10.1007/s12028-013-9830-5.
- Semenyutin V.B., Pechiborsch D.A., Aliev V.A. Transfer function assessment of dynamic cerebral autoregulation. Vestnik Voenno-meditsinskoy akademii 2013; 2(42): 180–188.
- Kornienko V., Pronin I. Diagnostic neuroradiology. Springer-Verlag Berlin Heidelberg; 2009, http://dx.doi.org/10.1007/978-3-540-75653-8.
- Bivard A., Levi C., Krishnamurthy V., Hislop-Jambrich J., Salazar P., Jackson B., Davis S., Parsons M. Defining acute ischemic stroke tissue pathophysiology with whole brain CT perfusion. J Neuroradiol 2014; 41(5): 307–315, http://dx.doi.org/10.1016/j.neurad.2013.11.006.
- Germano A., Merlo L., Campenn A., Trimarchi G., Baldari S. Pre- and postoperative cerebral perfusion assessment in chronic subdural hematoma. Abstracts from the 11th Symposium of the International Neurotrauma Society March 19–23, 2014, Budapest, Hungary. J Neurotrauma 2014; 31(5): A-1–A-73, http://dx.doi.org/10.1089/neu.2014.9937.
- Cao W., Campbell B.C., Dong Q., Davis S.M., Yan B. Relative filling time delay based on CT perfusion source imaging: a simple method to predict outcome in acute ischemic stroke. AJNR Am J Neuroradiol 2014; 35(9): 1683–1687, http://dx.doi.org/10.3174/ajnr.A3931.
- Yu Y.N., Ding X.F., Zhang S., Lou M. Thresholds of CT perfusion in predicting ischemic penumbra and infarct core in patients with acute ischemic stroke. Zhejiang Da Xue Xue Bao Yi Xue Ban 2014; 43(1): 7–13.
- Hong H.J., Kim Y.J., Yi H.J., Ko Y., Oh S.J., Kim J.M. Role of angiogenic growth factors and inflammatory cytokine on recurrence of chronic subdural hematoma. Surg Neurol 2009; 71(2): 161–166, http://dx.doi.org/10.1016/j.surneu.2008.01.023.









