Hyaluronic Acid in Treatment and Prevention of Postoperative Complications After Endoscopic Surgery for Benign Prostatic Hyperplasia
The aim of the investigation was to evaluate the clinical effect of URO-HYAL, a hyaluronic acid preparation, in the treatment of dysuric disorders and prevention of complications after transurethral endoscopic surgery for benign prostatic hyperplasia (BPH).
Materials and Methods. A randomized study was carried out in two groups of patients operated for BPH using transurethral enucleation with bipolar and bipolar transurethral resection of the prostate. In the postoperative period, 51 patients of the main group underwent 6 intravesical instillations of URO-HYAL, 150 patients of the control group received standard antibiotic therapy. The clinical effect was assessed 1, 3, 6, 12 months after the surgery on the basis of the complex urological examination results and adenoma bed bioptate histology.
Results. Histological examination of the adenoma bed bioptate of patients after endoscopic surgery for BPH has shown that intravesical administration of URO-HYAL in the postoperative period enables almost 2.5-fold reduction of the wound surface epithelization period. One month after the surgery there have been significantly less manifestations of dysuric disorders, higher life quality and no late postoperative cicatricial complications in the main group as compared to the control.
Conclusion. Treatment with URO-HYAL preparation after endoscopic surgery for BPH has been proved by our investigations to be pathogenically reasonable, clinically effective, and especially important for patients with a complicated course of BPH.
Dysuric disorders after endoscopic surgery for benign prostatic hyperplasia (BPH) are observed in the majority of patients on day 2–3 after urethral catheter withdrawal. These common postoperative symptoms regressing gradually within 1–2 weeks are not related, as a rule, to postoperative complications and are more often associated with the functional condition caused by electrothermal effect on the reflexogenic zone of the posterior urethra and the neck of the urinary bladder. At the same time in 11–25% of patients the irritative symptoms persist even in the late postoperative period. The reasons may be systemic microcirculatory disorders, detrusor hypoxia, hormonal imbalance, urinary bladder hyperactivity and, most often, acute inflammatory process in the prostate [1, 2].
To treat dysuric disorders the patients after surgery are administered standard antibiotic therapy, alpha-1-adrenoblockers, M-anticholinergic drugs, physiotherapy [3–6]. Hyperbaric oxygenation therapy [7] as well as instrumental methods [8] and bioregulatory peptides (Vitaprost preparation) [9–11] are used in some clinics. However, these types of treatment are not always effective for all the patients, and persisting urination disorders lower their life quality substantially. Therefore, search for new pathogenically reasonable methods of prevention and treatment of irritative urination disorders after endoscopic surgery for BPH is still an urgent problem of endourology.
From the viewpoint of pathogenesis of irritative disorders, the course of postoperative wound process in the adenoma bed after electroresection of the prostate is similar to a healing of a burn wound being under mechanical, chemical or biological effect of infected urine. Adenoma bed healing develops by its filling with granulation tissue, subsequent wound surface epithelialization and formation of new urothelium, which contributes to elimination of dysuria symptoms. In case of inflammation regeneration process is markedly delayed, rough cicatricial tissue is formed and the risk of such late complications as urinary bladder neck sclerosis, urethra stricture and urinary incontinence, increases [12].
The speed of wound healing largely depends on the intensity of formation of glycosaminoglycans and particularly hyaluronic acid that improves local microcirculation and activates migration and proliferation of cells participating in tissue regeneration. Local application of hyaluronic acid as tissue regeneration stimulator is pathogenically justified, and is already successfully applied in dermatology, ophthalmology, combustiology. URO-HYAL, a hyaluronic acid preparation, developed for the treatment of chronic recurrent and interstitial cystitis and painful bladder syndrome, is used in urology [13–17]. The findings of studying hyaluronic acid regenerative properties prove the advantages of its use in dysuria treatment after endoscopic surgery for BPH, which has determined the area of the present study.
The aim of the investigation was to evaluate the clinical effect of URO-HYAL, a hyaluronic acid preparation, in the treatment of dysuric disorders and prevention of complications after transurethral endoscopic surgery for benign prostatic hyperplasia.
Materials and Methods. The research was carried out on the basis of Urology Center of Railway Clinical Hospital on Gorky Station, Joint Stock Company “Russian Railway” (Russia) in 2013–2014. It was a randomized controlled study of clinical efficacy of URO-HYAL preparation in the treatment and prevention of complications in patients operated on for benign prostatic hyperplasia using transurethral enucleation with bipolar (TUEB) and bipolar transurethral resection of the prostate (B-TURP). URO-HYAL preparation developed by MKS Laboratories (Russia) and registered in Russia in 2010 is a protector of urinary bladder mucous membrane and is produced in the form of a sterile apyrogenic clear viscoelastic solution of sodium hyaluronate for intravesical administration.
In the postoperative period along with the traditional antibacterial and anti-inflammatory therapy the patients of the main groups (25 patients after B-TURP and 26 patients after TUEB) were administered 6 intravesical instillations of URO-HYAL: the first two procedures (20 mg (25 ml)) during hospital stay and the other four (40 mg (50 ml)) outpatiently once a week. Exposure time of the preparation in the urinary bladder was 1.5–2 h. The patients of the control groups (75 patients after B-TURP and 75 patients after TUEB) were treated according to the standard therapeutic scheme without hyaluronic acid.
The study was carried out in accordance with Declaration of Helsinki (adopted in June 1964 (Helsinki, Finland) and revised in October 2000 (Edinburgh, Scotland)) and was performed following approval by the Ethics Committee of Nizhny Novgorod State Medical Academy. Informed consent was received from every patient.
The necessary scope of observations was determined using the classic formula of non-repeated sampling and alternative distribution of the resulting characteristic, in our study it was the frequency of dysuric disorders after transurethral endoscopic surgery for BPH. In our center dysuria is observed in the early period after B-TURP and TUEB in 87.8±2.9% of patients on average [18]. According to calculations, the minimal scope of observations for our study amounted to 171.4 units, therefore a sample of 201 patients provided representativeness of the sampling population.
The patients with comparable basic parameters were selected into the main and control groups. The average age of the patients operated by B-TURP method was 65.5±1.2 years in the main group, and 65.2±1.2 years in the control (р=0.871), TUEB patients were 65.2±0.9 and 67.2±0.7 years old, respectively (р=0.080). The number of patients with BPH complications (presence of cystoma, cystic calculi, acute urinary retention) was the same in the main and control groups: 44.0% in every B-TURP group (р=0.842) and 28.0% in each TUEB group (р=0.921). The criteria recommended by the IV International Conciliation Committee on BPH (Paris, 1997) were used as assessment indexes:
1) assessment of BPH symptoms according to a 35-score scale of IPSS system with the focus on the symptom of emptying (obstructive — IPSSobstr) and the symptoms of collection (irritative — IPSSirrit);
2) assessment of life quality in connection with existing dysuria according to a 6-score scale (QoL);
3) maximum speed of urine flow according to uroflowmetry data (Qmax);
4) prostate volume according to US findings;
5) postvoid residual urine volume (RVR);
6) prostatic specific antigen level in blood serum (PSA);
7) the number and character of complications due to operative treatment.
Comparability of groups of patients under study according to the initial clinical data is given in Tables 1, 2. Clinical effect of the treatment was evaluated by comparing the resulting postoperative indices between the groups of patients 1, 3, 6, 12 months after the surgery. Adenoma bed epithelialization was assessed relying on the results of cystoscopy with TUR-biopsy and subsequent bioptate histology (8–14 histological slices) in the selected cohorts of patients: in 22 patients after the introduction of URO-HYAL and 26 after the standard therapy 1.5 months later, as well as in 18 patients from the control groups 2–4 months after the surgery.
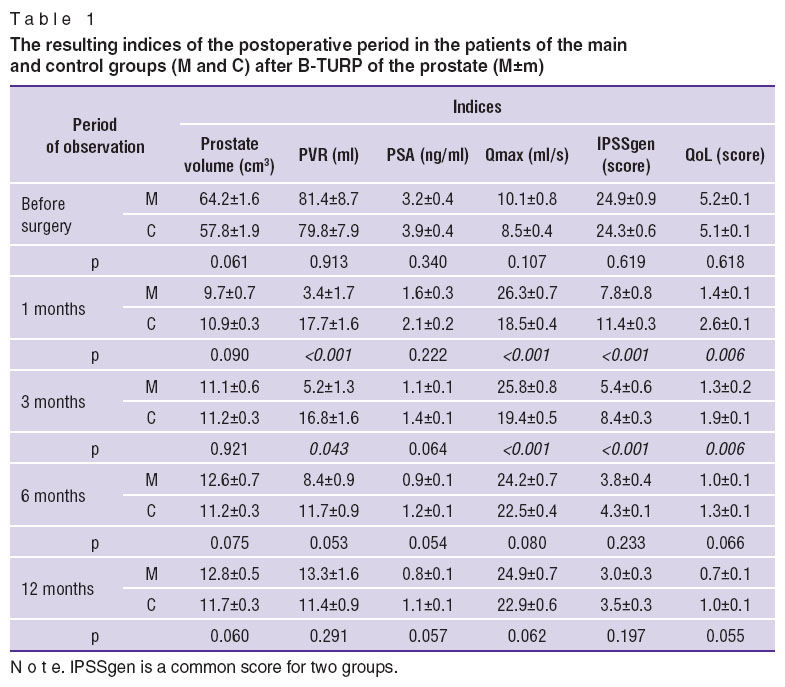 Table 1. The resulting indices of the postoperative period in the patients of the main and control groups (M and C) after B-TURP of the prostate (М±m) Table 1. The resulting indices of the postoperative period in the patients of the main and control groups (M and C) after B-TURP of the prostate (М±m)
|
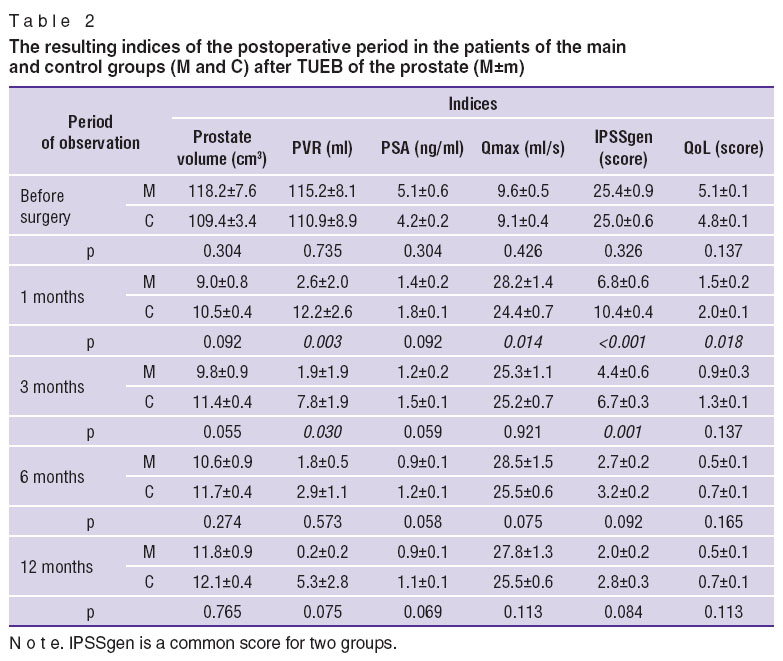 Table 2. The resulting indices of the postoperative period in the patients of the main and control groups (M and C) after TUEB of the prostate (М±m) Table 2. The resulting indices of the postoperative period in the patients of the main and control groups (M and C) after TUEB of the prostate (М±m)
|
The obtained results were statistically analyzed using software package Statistica 6.0 and Student’s t-test to identify the difference between mean and relative values, significance threshold being regarded as p≤0.05.
Results. Evaluation of the dynamics of symptoms according to IPSS scale showed significant decrease in their intensity in all the patients regardless of the surgery type, the most pronounced decrease being observed 1 and 3 months after the surgery (Figures 1, 2; See Tables 1, 2). At the same time the main groups demonstrated more intensive dynamics than the control: after B-TURP general IPSS score reduced 3.2 times vs 2.1 times in the control (р<0.001); after TUEB it reduced 3.7 times vs 2.4 times in the control (р<0.001). The revealed difference between the compared groups remained even 3 months after the surgery, but half a year later the index values equalized and the difference between them became insignificant.
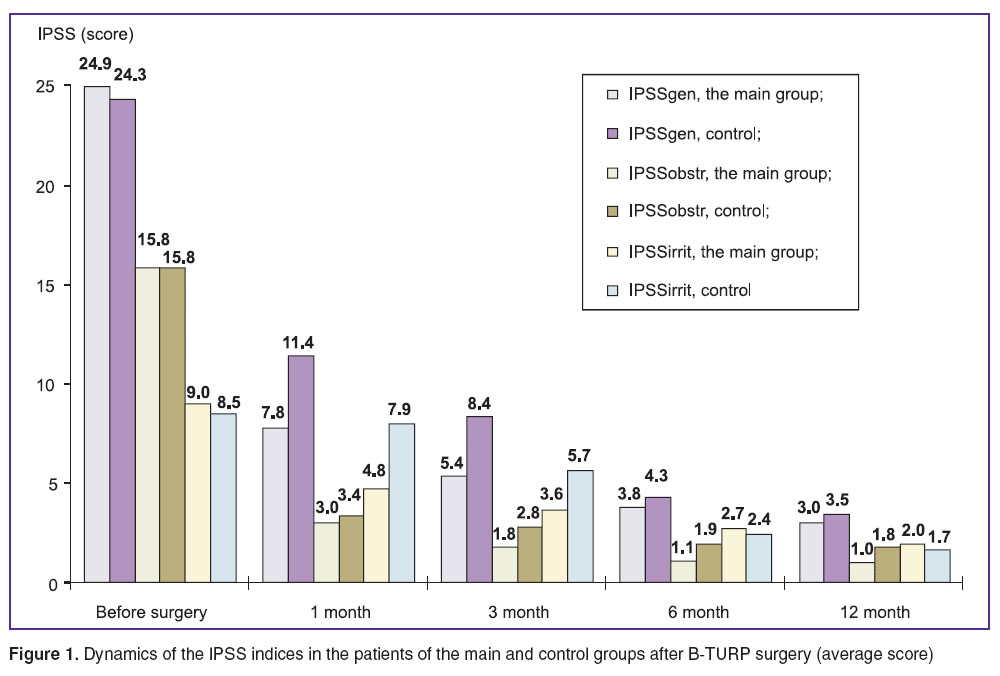 Figure 1. Dynamics of the IPSS indices in the patients of the main and control groups after B-TURP surgery (average score) Figure 1. Dynamics of the IPSS indices in the patients of the main and control groups after B-TURP surgery (average score)
|
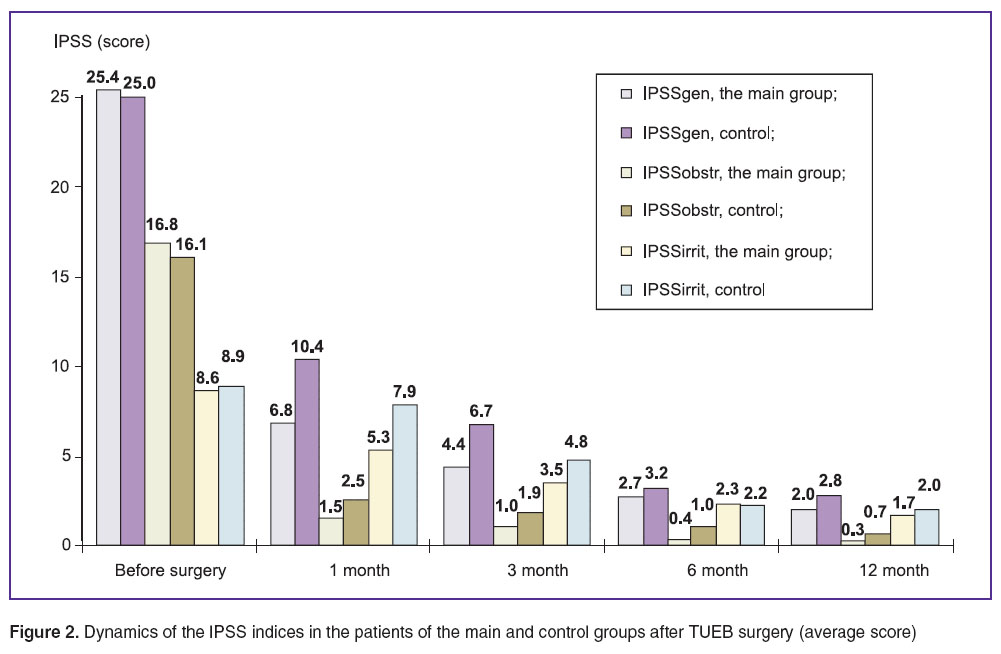 Figure 2. Dynamics of the IPSS indices in the patients of the main and control groups after TUEB surgery (average score) Figure 2. Dynamics of the IPSS indices in the patients of the main and control groups after TUEB surgery (average score)
|
IPSS analysis of the dynamics of the symptoms of emptying and collection shows that operative treatment leads to practically complete elimination of obstructive symptoms in all the patients in the nearest postoperative period. One month after B-TURP infravesicular obstruction signs decrease 4.5–5.0 times without significant difference of indices between the compared groups. After TUEB the mean score of obstruction decreases 11 times during the first month in the main group (from 16.8±0.7 to 1.5±0.3), and only 6 times in the control (from 16.1±0.4 to 2.5±0.2; р=0.05). In subsequent observation periods the index difference between the compared groups of patients levels.
The most significant difference between the studied groups of patients was determined by IPSS indices of irritative symptoms, it remained up to 3 months after both types of surgery. At the same time symptoms of collection altered slightly in the control groups and significantly decreased in the groups of patients having received a course of URO-HYAL instillations. After B-TURP IPSSirrit index in the main group, reducing two-times from the initial value, amounted to a score of 4.8±0.4 after 1 month, and to a score of 3.6±0.2 after 3 months, while in the control reduction was insignificant: up to a score of 8.0±0.3 after 1 month and to a score of 5.7±0.2 after 3 months (р<0.001). Irritative symptoms after TUEB in the main group decreased 1.6 times after 1 month — up to a score of 5.3±0.4, after 3 months — up to a score of 3.5±0.3, while in the control the dynamics was less prominent — up to a score of 7.9±0.3 and 4.8±0.2, respectively (р<0.001).
Persistence of irritative symptoms after surgery in the control group worsened the quality of their life (See Tables 1, 2). After 1 month QoL index was 1.8 times lower in the control group after B-TURP than in the main group (р=0.006), and statistically significant difference remained up to 3 months. Between TUEB groups of patients the QoL difference was expressed only 1 month after the surgery (a score of 1.5±0.2 and 2.0±0.1; р=0.018), at a later stage life quality indices equalized in the compared groups.
Similar tendencies were noticed when comparing uroflowmetry indices and postvoid residual urine volume. After the operative intervention positive dynamics of Qmax and PVR was observed in all the patients, however, in the groups after URO-HYAL instillations it was significantly more expressed and the indices difference remained up to 3 months. Qmax increased 2.6 times (to 26.3±0.7 ml/s) 1 month after B-TURP in the main group, and 2.2 times in the control group (to 18.5±0.4 ml/s; р<0.001); after TUEB it grew 2.9 times in the main group (to 28.2±1.4 ml/s), and 2.7 times in the control (to 24.4±0.7 ml/s; р=0.014). In the same observation period PVR decreased 24 times (to 3.4±1.7 ml) in the main group, and only 4.5 times (to 17.7±1.6 ml; р<0.001) in the control; in the main group after TUEB the decrease was 44 times (to 2.6±2.0 ml), and only 9 times in the control (to 12.2±2.6 ml; р=0.003).
Comparing the dynamics of the rest clinical indices including РSA and prostate volume levels, presented in Tables 1, 2, revealed no significant differences between the main and control groups of patients, since the given parameters characterize the presence of massive processes in the prostate and operative treatment radicality and are not sensitive to the results of postoperative treatment of dysuria.
The analysis of postoperative complications occurrence showed that the patients receiving URO-HYAL did not develop hemorrhages in the early postoperative period, yet they were seen in the control groups: in 5.3±2.6% of cases (р=0.043) after B-TURP and in 2.7±1.9% of patients (р=0.152) after TUEB (Table 3). As to the frequency of early infectious inflammatory complications, no statistical difference between the compared groups was established. Single cases of acute orchiepididymitis were seen in the patients of both the main (3 out of 51) and the control group (4 of 150) and were generally related to the complicated BPH course, presence of inflammation signs and high concentration of microorganisms (more than 105 CFU/ml) in the urine test before the surgery. There was a single case when a patient from the B-TURP group with acute urine retention and repeated urinary catheterization for several days before the surgery was operated on, in 6 other cases the operated patients had cystoma.
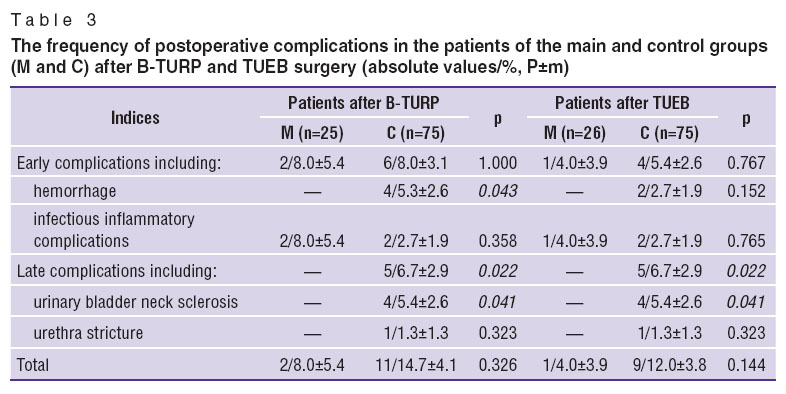 Table 3. The frequency of postoperative complications in the patients of the main and control groups (M and C) after B-TURP and TUEB surgery (absolute values/%, Р±m) Table 3. The frequency of postoperative complications in the patients of the main and control groups (M and C) after B-TURP and TUEB surgery (absolute values/%, Р±m)
|
Late postoperative complications after endoscopic surgery occurred only in the control groups with the same frequency — 6.7±2.9% (5 of 75) of cases after B-TURP and TUEB and manifested themselves by the presence of a pathological cicatricial process in the neck of the urinary bladder (5.4±2.6%) or the urethra (1.3±1.3%). As a rule, these complications occurred in patients with BPH complications and initial inflammatory signs in the urine tests. After administration of URO-HYAL in B-TURP and TUEB groups no late postoperative complications were found (р=0.022).
In order to confirm the obtained clinical results histologically the operated patients underwent cystoscopy with TUR-biopsy of the tissue samples from the adenoma bed at different times of the postoperative period. According to histology data, after completing the course of URO-HYAL introduction (1.5 months after the surgery) 86.4±7.3% of patients (19 of 22) after B-TURP 100.0% (13 of 13) and after TUEB 66.7% (6 of 9) showed complete surface epithelialization, transitive epithelium covered the whole surface of the taken adenoma bed segment. In the stroma there were areas of neoangiogenesis with a great number of closely located small vessels. In 3 out of 9 TUEB patients (33.3%) epithelialization was not fully completed after 1.5 months: in 2 patients by 50% (epithelialization signs in 5 of 7 histological slices) and in one patient by 63% (5 of 8 slices).
At the same time in 80.8±7.7% of patients (21 of 26) on the standard postoperative therapy (64.3% (9 of 14) after B-TURP and 100% (12 of 12) after TUEB) the signs of adenoma bed surface epithelialization were absent in histological slices 1.5 months after the surgery, which demonstrated a significant difference in comparison with the group of patients who received URO-HYAL (0% with the absence of epithelialization signs; р<0.001). The surface of segments (bioptates) presented granulation tissue, sometimes with massive necrosis and lympholeucocytic infiltration. In 5 out of 14 control patients (35.7%) after B-TURP epithelialization was incomplete: in 2 cases it was complete by 42% (in 5 slices out of 12) and in 3 cases by 30% (3 slises out of 10).
To make the terms of complete epithelialization of adenoma bed surface more precise after standard postoperative therapy 18 patients (9 after B-TURP and 9 after TUEB) underwent histological examination at a later period. It was established that 2 months after the surgery the picture of complete epithelialization was seen only in 11.1% (1 of 9) of B-TURP patients, after 3 months in other 22.2% (2 of 9) of patients from the same group, after 4 months in 33.3% (3 of 9) of B-TURP patients and in 44.4% (4 of 9) of TUEB patients. The rest 33.4% of patients after B-TURP and 55.6% after TUEB showed partial surface epithelialization or its absence after 4 months.
Discussion. The analysis of histological results in patients operated on for BPH with the use of different endoscopic methods has demonstrated that hyaluronic acid application in the postoperative period significantly fastens the processes of granulation tissue growth with subsequent epithelialization of the adenoma bed. In case of using the standard postoperative therapy scheme complete epithelialization of the adenoma bed occurs only after 4 months in most patients. Introducing URO-HYAL intravesically we achieved epithelialization of adenoma bed already in 1.5 months in all the B-TURP patients, and in 2 out of 3 patients operated by the TUEB method. In B-TURP the volume of the removed tissue is less, consequently the area of the adenoma bed is smaller, so epithelialization goes faster than in the patients after TUEB.
Fast recovery of the urothelium after treatment with URO-HYAL contributes to the reduction of dysuric manifestations and complications in the early postoperative period, resulting in a faster normalization of life quality indices of the operated patients. One month after the surgery the patients of the main groups have significantly lower indices of IPSS irritative symptoms and postvoid residual urine volume, higher uroflowmetry indices and no hemorrhages in comparison with the control. Moreover, quick epithelialization of the wound surface prior to cicatrical tissue formation allows to avoid such late postoperative complications as urinary bladder neck sclerosis and urethra stricture. Therefore, the use of hyaluronic acid is especially important for patients with a complicated course of BPH (the presence of cystoma, cystic calculi, acute urine retention) and high risk of developing postoperative complications.
Conclusion. Treatment with hyaluronic acid preparation URO-HYAL after endoscopic surgery for benign prostatic hyperplasia is pathogenically reasonable and clinically effective as it enables the reduction of dysuric disorders, prevention of postoperative complications of sclerotic character, thus improving the quality of operated patients’ life.
Study Funding and Conflicts of Interest. This study was not supported by any financial sources, and there is no conflict of interests associated with the research.
References
- Martov A.G., Merinov D.S., Kornienko S.I., et al. Postoperative urological complications in transurethral electrosurgical interventions on the prostate for adenoma. Urologiya 2006; 2: 25–31.
- Al-Shukri S.Kh., Tkachuk I.N. The prophylactics of irritational disorders of urination after transurethral resection of prostate gland in patients with benign hyperplasia of prostate gland. Nefrologiya 2008; 12(4): 67–71.
- Souverein P.C., Erkens J.A., de la Rosette J.J., Leufkens H.G., Herings R.M. Drug treatment of benign prostatic hyperplasia and hospital admission for BPH-related surgery. Europ Urol 2003; 43(5): 528–534, http://dx.doi.org/10.1016/S0302-2838(03)00089-7.
- Oelke M., Bachmann A., Descazeaud A., Emberton M., Gravas S., Michel M.C., N’Dow J., Nordling J., de la Rosette J.J. Guidelines on male lower urinary tract symptoms (LUTS), including benign prostatic obstruction (BPO). Geneva: EAU; 2012, http://uroweb.org/wp-content/uploads/11_Male_LUTS.pdf.
- Markov A.V., Lukianov I.V., Loran О.В. Complex therapy of irritative voiding disorders after transurethral resection of the prostate and adenomectomy. Urologiya 2007; 4: 41–44.
- Urologiya. Klinicheskie rekomendatsii. 3-e izd [Urology. Clinical guidelines. 3rd ed.]. Moscow: GEOTAR-Media; 2014.
- Shormanov I.S., Ryzhkov A.I. Hyperbaric oxygenation in the treatment of urination disorders after transurethral resection of benign prostatic hyperplasia. Fundamentalnie issledovania 2011; 1: 205–212.
- Loran О.В., Lukiyanov I.V., Markov A.V. Combined therapy of voiding irritative disorders after surgical treatment of benign prostatic hyperplasia with Andro-Gin. Urologiya 2005; 3: 15–18.
- Kamalov A.A., Efremov E.A., Dorofeev S.D., Mel’nik Ya.I., Okhobotov D.A. Vitaprost forte in the treatment of patients with prostatic adenoma. Urologiya 2007; 3: 39–47.
- Yaroshenko V.P., Miller A.M. Irritational disorders of urination after transurethral electroresection in patients with benign prostatic hyperplasia. Effektivnaya farmakoterapiya. Urologiya i nefrologiya 2011; 1: 27–28.
- Tkachuk V.N., Tkachuk I.N. Efficacy of Vitaprost forte in the treatment of patients with prostatic adenoma. Urologiya 2014; 2(13): 63–67.
- Zakhmatov Yu.M., Varentsov G.I., Otvetchikov A.I., Kornev A.I. Dinamika IPSS posle razlichnykh vidov operativnogo lecheniya DGPZh. V kn.: Materialy X rossiyskogo s”ezda urologov [IPSS dynamics after different types of surgery for BPN. In: Materials of the 10th Russian Conference of Urologists]. Moscow; 2002; p. 112–114.
- Kudrjavcev Ju.V., Kirpatovskiy V.I., Perepanova T.S., Khazan P.L. Glycosaminoglycans stabilizer zinc hyaluronate use in experimental modeling of acute bacterial and interstitial cystitis. Eksperimental’naya i klinicheskaya urologiya 2011; 1: 39–44.
- Glybochko P.V., Alyaev Yu.G., Gadzhieva Z.K., et al. Application of hyaluronic acid in the treatment of chronic cystitis. Effektivnaya farmakoterapiya. Urologiya i nefrologiya 2011; 5: 30–35.
- Morales A., Emerson L., Nickel J.C., Lundie M. Intravesical hyaluronic acid in the treatment of refractory interstitial cystitis. J Urol 1996; 156(1): 45–48, http://dx.doi.org/10.1016/S0022-5347(01)65933-0.
- Constantinides C., Manousakas T., Nikolopoulos P., Stanitsas A., Haritopoulos K., Giannopoulos A. Prevention of recurrent bacterial cystitis by intravesical administration of hyaluronic acid: a pilot study. BJU Int 2004; 93(9): 1262–1266, http://dx.doi.org/10.1111/j.1464-410X.2004.04850.x.
- Lipovac M., Kurz C., Reithmayr F., Verhoeven H.C., Huber J.C., Imhof M. Prevention of recurrent bacterial urinary tract infections by intravesical instillation of hyaluronic acid. Int J Gynaecol Obstet 2007; 96(3): 192–195, http://dx.doi.org/10.1016/j.ijgo.2006.11.025.
- Sevryukov F.A. Kompleksnye mediko-sotsial’nye i kliniko-ekonomicheskie aspekty profilaktiki i lecheniya dobrokachestvennoy giperplazii predstatel’noy zhelezy. Avtoref. dis. … dokt. med. nauk [Complex medical-social and clinical-economic aspects of prevention and treatment of benign prostatic hyperplasia. DSc Thesis]. Moscow; 2012.









