Biochip-SER Test System for Fluorescent Immunocytochemical Analysis of Ep-CAM Antigen Expression in Effusions and Washes
The aim of the study was to evaluate the Biochip-SER test system for its ability to measure the expression of Ep-CAM antigen by fluorescent immunocytochemistry.
Materials and Methods. We conducted 64 cytological, 64 standard immunocytochemical (SICC) and 64 fluorescent immunocytochemical (FICC) tests using the Biochip-SER test system and samples from 59 patients (45 effusions and 19 peritoneal washings). The study was performed in 4 stages: cytological examination, SICC, FICC using the Biochip-SER system, and control cytological study by the Biochip-SER system. The SICC was performed using the monoclonal antibody (MAB) to the epithelial antigen Ep-CAM; FICC was performed using the MAB to the epithelial antigen Ep-CAM conjugated to the Alexa Flour 488 fluorochrome.
Results. FICC test performed using the Biochip-SER test system, showed 100% diagnostic sensitivity and 89% specificity.
Conclusion. FICC test carried out with MAB to the Ep-CAM antigen conjugated with Alexa Flour 488 using the Biochip-SER system is a reliable method for diagnosing tumors by testing effusion fluids, which allows us to recommend this system for practical use in specialized institutions and primary points of care.
Introduction
Detection of metastatic tumor cells in exudates is highly important because it allows for early diagnosis and a timely started treatment. Serous cavities of a human body are lined with epithelial cells of mesenchymal origin (mesothelium). In disease (neoplasia, infectious or systemic diseases), the mesothelium becomes polymorphic and even atypical due to its reactive proliferation [1]. The morphological variability of reactive mesothelium complicates the differential diagnosis between malignant mesothelioma and carcinoma metastases, which calls for using additional diagnostic means.
In a healthy person, there is about 10 ml of serous fluid in the pleural cavity, about 1–2 ml — in the pericardial space, and up to 50 ml — in the peritoneal cavity [2]. It is commonly accepted that an excess volume of fluid in the cavities is a sign of pathology and can serve an indication for a diagnostic puncture.
Malignant diseases are often accompanied by effusion into the pleural and peritoneal cavities; in such exudates, tumor cells can be detected. In men, the detection rate is 49% in lung cancer, followed by leukemia and malignant lymphomas (21%), carcinomas of the digestive system (7%) and the genitourinary system (6%). In women, pleural and peritoneal exudates are detected twice more often, especially with the progression of breast (37–50%) and ovarian (20%) cancer, and less likely with malignant lymphomas (8%) and GI carcinomas (4%) [3].
By now, cytological examination is the only diagnostic means to confirm or refute the malignant nature of the exudate, however, its reliability varies from 60 to 96% [2, 4, 5].
When assessing the morphology of serous effusions, the presence of polymorphic cells with severe nuclear atypia and characteristic cell clusters (acinar, micro-papillar, spherical, etc.) enables the diagnosis of a malignant tumor with confidence. However, the diverse cellular composition of the exudate — the presence of proliferating mesothelial cells, lymphoid and histiocytic-macrophage elements, leukocytes, and tumor cells morphologically similar to the cells of the mesothelium — may raise doubts about the nature of the effusion.
Difficulties in discerning between the reactive mesothelium, mesothelioma or metastatic cancer in most cases can be overcome using additional methods: immunocytochemistry, cytogenetic analysis, flow cytometry, electron microscopy, etc. [6–8].
In immunocytochemistry, monoclonal antibodies (MAB) to the surface epithelial antigen Ep-CAM (clone Ber-EP4) are often used to resolve controversial diagnostic situations. Ep-CAM is a transmembrane protein consisting of two molecules of glycoproteins with molecular masses of 34 and 39 kDa; the protein is found in the membrane and the cytoplasm of normal epithelial cells, carcinoid cells and carcinomas of various origins [9, 10]. Ep-CAM is not expressed in most non-epithelial tumors, in mesothelial cells, hepatocytes or lymphocytes. In combination with other markers, Ep-CAM can be used to confirm the epithelial origin of a tumor in the differential diagnosis between adenocarcinoma (AC) and mesothelioma [11, 12].
Immunocytochemical assays using MAB to Ep-CAM showed high sensitivity, specificity and predictive power in detecting A: those were 80, 94 [13], and 96%, respectively [14]. In studies conducted in the Russian Federation, using the Ep-CAM marker increased the sensitivity and specificity of cytological diagnosis of AC to 96 and 99%, respectively [15].
Promising results have been obtained using Ep-CAM in the differential diagnosis between AC and mesothelioma: the reaction is positive in 100% of adenogenic lung carcinomas, in 100% of squamous cell carcinomas, in 93% of non-lung carcinomas, in 67% of urothelial carcinomas and in 84% of metastatic ACs with unknown primary tumor location. In mesothelioma cells, the expression of Ep-CAM was detected in 18–26% of observations [16, 17], and this expression was focal in nature, i.e., it was observed only in part of the tumor cells.
Today, immunocytochemical studies include the method of fluorescent immunocytochemistry (FICC), which allows for intraoperative testing of exudates, thanks to its time-saving technique and confirmed efficacy. Thus, Japanese authors [18] compared different immunocytochemical modalities: standard (SICC), standard and urgent intraoperative FICC using 64 fluid samples (35 washings from peritoneal cavities and 29 ascitic effusions) obtained from patients with various non-neoplastic pathologies and malignant diseases. In the SICC and FICC assays, they used the following markers: Ber-EP4, CEA, EMA, and MOC-31; of those, the Ber-EP4 and MOC-31 clones were the most significant in diagnosing the tumorous nature of the effusion. These markers were highly expressed in AC cells, but completely absent in cells of the reactive mesothelium: in 92% of the AC cases (12 of 13), the cells were Ber-EP4/MOC-31 positive.
According to our own data, the use of SICC and FICC with Ep-CAM (Ber-EP4) increases up to 100% the sensitivity and specificity of the cytological method in testing effusions and washes [5].
Taking into account the high sensitivity and specificity of the MAB to Ep-CAM (Ber-Ep4 clone), this marker was selected for this study to identify AC cells using SICC and FICC.
In order to improve cytological and immunocytochemical methods, we developed a test system called Biochip-SER. This system represents a high-tech medical product for conducting FICC-based analysis and research [19]. It consists of two main parts: working and functional (Figure 1). The working part is a transparent glass pad with dimensions of 25.4×76.2 mm and a thickness of 1 mm. The pad is coated with a positively charged material; it is divided into 15 equal wells by means of a plastic grid. Each well contains MAB to Ep-CAM (Ber-EP4 clone) conjugated with Alexa Flour 488 fluorochrome with an excitation waveband of 468–509 nm and emission at 504–541 nm. To preserve antibodies in a humid environment, 0.1 μl of PBS (phosphate buffer) is added to each cell and a hydrophobic film is applied on top of the working surface, preventing it from drying out. Depending on the density of tumor cells in the biological sample, the number of cells added to the test system may vary. If the number of tumor cells is too small, all 15 biochip wells can be used.
|
Figure 1. |
A certain part of the biochip surface has no specific coating; it is intended for marking (QR code) and handling in the course of manipulations.
The aimof the study was to evaluate the Biochip-SER test system for its ability to measure the expression of Ep-CAM antigen by fluorescent immunocytochemistry.
Materials and Methods
We conducted 64 cytological, 64 standard immunocytochemical (SICC) and 64 fluorescent immunocytochemical (FICC) tests using the Biochip-SER system and samples from 59 patients with tumor and non-tumor pathology. The study included 8 men (aged 33–67 years) and 51 women (aged 29–88 years) and conducted in accordance with the Helsinki Declaration (2013); the protocol was approved by the Ethics Committee of the N.N. Blokhin Russian Cancer Research Center. Informed consent was obtained from each patient. Cellular components of 45 effusions (26 ascites, 17 pleurisy samples, 2 pericardial effusions) and 19 peritoneal washings were tested. Two patients were sampled twice, and three patients had pleural and peritoneal effusions (Table 1). Of the 59 patients, 57 individuals (96.6%) had oncological history (serous papillary ovarian cancer, borderline ovarian tumor, endometrial AC, breast cancer, colon cancer, gastric cancer, lung AC, mesothelioma, small cell lung cancer), in 2 patients (3.4%) no tumor was detected (1 case of hepatic echinococcosis and 1 — uterine tube endometriosis). Among patients with tumor pathology, 7 (12.3%) were diagnosed with primary multiple malignant neoplasms. Only in 42 of 59 patients, the presence/absence of the tumor spread into the peritoneum/pleura was histologically verified; in two patients with non-neoplastic pathology (endometriosis, echinococcosis) the diagnoses were also confirmed.
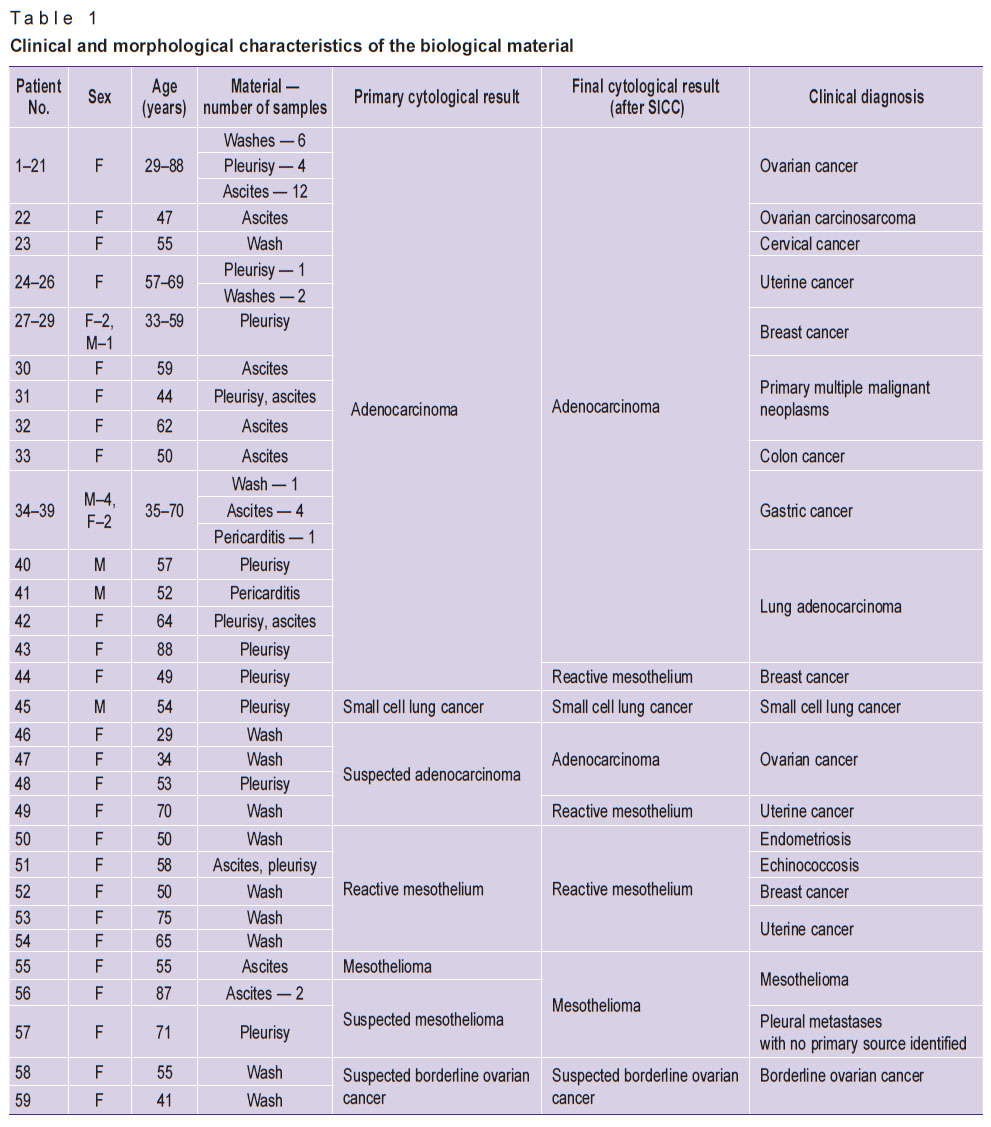 |
Table 1. Clinical and morphological characteristics of the biological material |
Although Ep-CAM was known for its highest expression in AC cells, its expression in other tumors and cells of the reactive mesothelium was also of interest.
We considered all the studied material to be informative since we used only the sediments with high cellularity for testing by the SICC and FICC.
The study was carried out in four stages: stage 1 — cytology; stage 2 — SICC; stage 3 — FICC with the Biochip-SER test system; stage 4 was a control cytological examination using the Biochip-SER system.
For the cytological, SICC and FICC studies, a concentrated cell suspension was used; that was prepared by centrifuging the sediment formed by spontaneous cell sedimentation while the biological fluid sample was standing. The precipitate was placed in a 10 ml centrifuge tube and spun at 2000 rpm for 10 min in an OPN-3M centrifuge (ELMI Ltd., Latvia). The supernatant was decanted, leaving up to 1 ml of cell suspension. The contents of the tubes were resuspended or vortexed to obtain a homogeneous cell suspension, which was then placed (in a volume of 50–80 μl, depending on cell density) into Cytospin-3 cytocentrifuge cuvettes (Thermo Scientific Shandon, United Kingdom) and spun at 1500 rpm for 10 min.
A series of monolayer smears was prepared: for the cytological study, 2 smears were stained by Romanovsky–Leishman; additional 2 smears were tested by SICC with MAB to the Ep-CAM epithelial antigen, clone Ber-EP4 (Dako, USA). The presence of membrane staining in tumor cells indicated a positive expression of Ep-CAM.
To confirm the diagnosis and differential diagnosis, in several cases (n=9), the SICC study was performed with MAB to the WT-1 antigen, clone 6F-H2, titer 0.7:100 (Cell Marque Corp., USA), MAB to calretinin, Calret clone, titer 1:100 (Dako, United States), MAB to mesothelin, clone NCL-L-MESO, titer 1:40 (Novocastra Laboratries, UK), MAB to HBME-1 mesothelial antigen, HBME-1 clone, titer 1:40 (Cell Marque Corp., USA), MAB to desmin, clone D33, titer 1:100 (Cell Marque Corp., USA), MAB to TTF-1, clone G7G3/1, titer 0.7:100 (Cell Marque Corp., USA), MAB to CK7, OV-TL 12/30 clone, titer 0.7:100 (Cell Marque Corp., USA), MAB to synaptophysin, clone MRQ-40, titer 0.7:100 (Cell Marque Corp., USA), MAB to the epithelial-related antigen, MOC-31 clone, titer 1:60 (Dako, United States). All SICC assays were performed using a BenchMark ULTRA immunohistostainer (Ventana, USA).
To perform FICC using the Biochip-SER system, a 10% solution of rheopolyglucin was added to the residual cell suspension at a ratio of 1:9 (in order to reduce the background staining and leveling the autofluorescence effect) and centrifuged again for 10 min. The supernatant was removed to leave a residual volume of 0.6–0.8 ml. After removing the protective film from the biochip surface, the cell suspension was added in a volume of 30 μl to each well. When the biological material was added to the wells, a direct immunocytochemical reaction “antigen–antibody” took place, and the product was determined by fluorescence. For the uniform distribution of the material and acceleration of the “antigen–antibody” reaction, the contents of the wells were thoroughly mixed, and the biochip was incubated for 30 min in a hybridizer (using a thermostat or thermo shaker is also possible). Then, the reaction products were evaluated using an Axio Imager Z2 fluorescence microscope (Carl Zeiss, Germany) with FICC and DAPI filters.
The expression of the Ep-CAM antigen was measured in each of the wells of the test system according to the following criteria:
the presence or absence of specific membrane luminescence in the tumor cells;
the number of reacting cells;
fluorescence intensity.
Subsequently (stage 4), the biochip was stained in the traditional way (according to Leishman) for the control cytological examination. In all cytological preparations, the diversity of the cell composition, the density of tumor cells in the material, the characteristic morphological features and the architectonics of the tumor were evaluated. Microscopy was performed using an Eclipse Ci light microscope (Nikon, Japan) at 100, 200, 400, and 1000 magnifications.
Results and Discussion
Cytological studies (stage 1). The results can be grouped as follows.
1. Confident conclusion about the presence of tumor cells (n=51). The biological sample was highly cellular. In accordance with the nosology, characteristic morphological features of tumor cells and their clusters were observed.
2. The presence of tumor cells suspected (n=7). This uncertain conclusion was due to:
the presence of isolated cells morphologically similar to tumor cells (n=2);
heterogeneous cellular composition with a pronounced lymphocytic-histiocytic reaction (n=2);
cells of the reactive proliferating mesothelium suspected of mesothelioma (n=2), or clusters of tumor cells that are difficult to ascribe to either AC or mesothelioma (n=1).
3. Confident conclusion about the absence of tumor cells (n=6). In all observations of this group, the cytograms were represented by unstructured clusters and layers of mesothelium cells.
The SICC results (stage 2). The use of SICC allowed us to confirm the cytological diagnosis in 56 cases, to clarify it in 6 and to avoid overdiagnosing — in 2 cases (see Table 1).
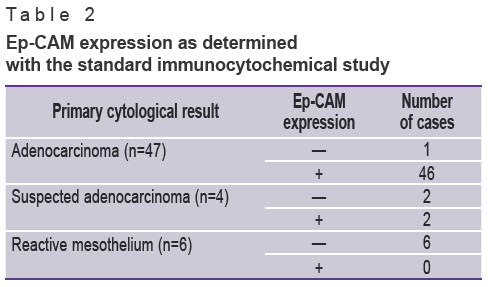
To assess the sensitivity and specificity of the cytological method in detecting AC, we excluded those cases where mesothelioma was confidently or highly likely diagnosed (n=4), tumors with borderline malignancy (n=2) and small cell cancers (n=1). Therefore, of 64 cases subjected to cytological analysis, we selected 57 for the SICC studies. The SICC test with the MBA to Ep-CAM (n=57) allowed us to confirm the cytological conclusion “adenocarcinoma” in 46 cases, and also to confirm 2 observations earlier defined as suspicious of AC (Table 2).
|
|
Since there were no false-negative cytological results, the sensitivity of cytological diagnosis was 100%. The group of false-positive cytological findings included 2 observations suspicious of AC that were not confirmed in the SICC, as well as one case with a confident conclusion about a metastasis of adenogenic cancer. Thus, the specificity of the cytological method was only 67%. However, this figure can only be considered as preliminary because the number of patients was too small to make generalizations.
In borderline ovarian tumors (n=2), positive expression of Ep-CAM was observed in both cases. In all cases with affirmative or presumptive conclusions about mesothelioma (n=4), as well as dissemination of small cell lung cancer in the pleura, the reaction with Ep-CAM was negative. The diagnosis of epithelioid cell mesothelioma was confirmed by SICC results showing a positive expression of calretinin, mesothelin, WT-1, HBME and a negative expression of MOC-31 and desmin. In our SICC assay, small cell carcinoma was characterized by a positive expression of TTF-1 and synaptophysin (previously, histogenesis of this tumor was confirmed immunohistochemically).
FICC studies using the Biochip-SER test system (stage 3). FICC performed with the Biochip-SER system showed a 100% diagnostic sensitivity: in all cases of AC, confirmed by the SICC, positive expression of Ep-CAM antigen was detected. The test specificity was 89%; in just one observation, the results of the FICC and SICC did not match each other (a positive reaction was found only with the biochip). In this specific case, a later dissemination of the tumor was histologically detected, which confirmed the FICC result.
It is important to add a few comments that may be useful while working with the Biochip-SER test system. Thus, due to the impact of radiation or chemotherapy, tumor cells undergo dystrophic and degenerative changes, which affect the fluorescence pattern of the membrane-bound Ep-CAM. The fluorescent signal, therefore, may have a varying intensity (from low to moderate). This phenomenon may complicate the detection and identification of tumor cells.
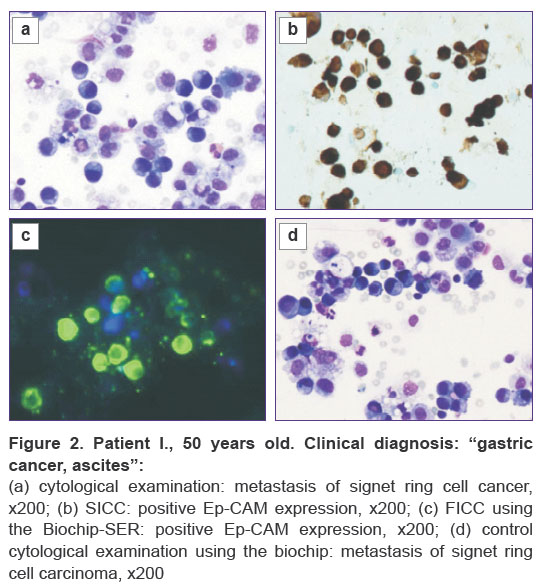
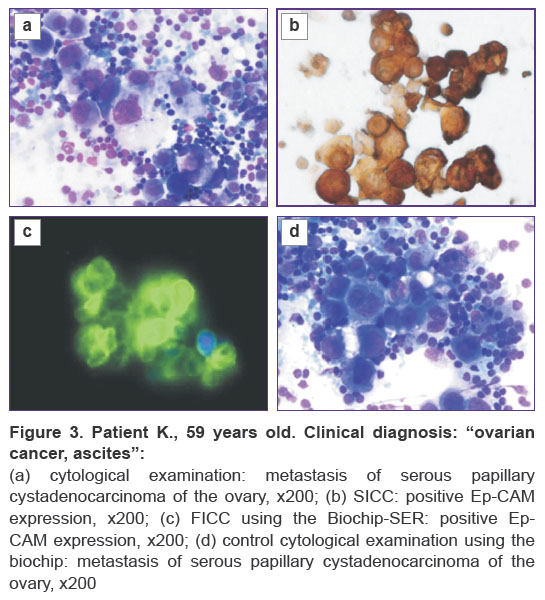
Control cytological study using the Biochip-SER system. In this study, we noted a good preservation of tumor cell morphology and cell cluster architectonics. The distribution of cellular elements in the chip wells was not uniform: the largest number of cells accumulated in the corners of the wells; this is well illustrated by the examples shown in Figures 2 and 3.
|
Figure 2. Patient I., 50 years old. Clinical diagnosis: “gastric cancer, ascites”: (a) cytological examination: metastasis of signet ring cell cancer, x200; (b) SICC: positive Ep-CAM expression, x200; (c) FICC using the Biochip-SER: positive Ep-CAM expression, x200; (d) control cytological examination using the biochip: metastasis of signet ring cell carcinoma, x200 |
Thus, the present study showed highly comparable results of the FICC and SICC tests in probing the expression of Ep-CAM. Besides, using the Biochip-SER test system adds more advantages to the FICC assay:
time saving — the test takes about 60 min including the sample preparation (vs. 180 min in SICC);
the ability to perform a control cytological test using the same chip: after FICC it is stained in the traditional way;
the fluorochromes used in this study have a long term fluorescence;
low cost, saving reagents and consumables;
there is no need to use a visualization system or diaminobenzidine (which is carcinogenic);
possible use of telemedicine — the pre-analytical stage can be conducted by a trained nurse at a primary care point; later the scanned image can be transmitted to a specialized reference center.
Conclusion
In this study, we demonstrate a novel technology to facilitate the differential diagnosis of metastatic adenocarcinomas, mesotheliomas, and reactively altered mesothelium by testing biological fluids from serous cavities. The proposed Biochip-SER test system combined with the fluorescent technique and the use of MAB to Ep-CAM has a number of advantages in comparison with the current FICC assay commonly used for diagnosing a tumor process in effusion fluid. The results allow us to recommend the Biochip-SER for diagnostic use both in specialized institutions and at the primary care centers.
Research funding. This work was carried out with the support of the SPE Biochip.
Conflict of interest. The SPE Biochip did not intervene in the course of the research and did not influence its results.
References
- Semenov D.A., Tseluyko S.S. Histophysiology of the pleural cavity and pleural effusion. Dal’nevostochnyy meditsinskiy zhurnal 2012; 2: 140–144.
- Dolgov V.V., Shabalova I.P., Mironova I.I., Djangirova T.V., Korotaev A.L. Vypotnye zhidkosti. Laboratornoe issledovanie [Serous effusions. Laboratory diagnostics]. Moscow: Triada; 2006.
- Gluzman D.F., Sklyarenko L.M., Nadgornaya V.A., Kryachok I.A. Diagnosticheskaya immunotsitokhimiya opukholey [Diagnostic immunocytochemistry of tumors]. Kiev: Morion; 2003.
- Shidham V.B., Atkinson B.F. Cytopathologic diagnosis of serous fluids. Elsevier Saunders; 2007.
- Savostikova M.V., Furminskaya E.Yu., Fedoseeva E.S., Kudaibergenova A.G. The fluorescent immune cytochemical analysis of exudations and washouts from serous cavities under intra-operational cytological diagnostic. Klinicheskaia laboratornaia diagnostika 2017; 62(12): 742–745.
- Lazarev A.F., Grigoruk O.G., Bazulina L.M., Muzalevskiy P.N., Kravtsov V.Yu. Pleural mesothelioma: etiology, incidence, diagnosis, treatment and survival. Rossiyskiy onkologicheskiy zhurnal 2013; 5: 15–20.
- Davidson B. Malignant nonhematological effusion characterization by flow cytometry. Acta Cytol 2016; 60(4): 365–371, https://doi.org/10.1159/000447687.
- Bolgova L.S., Marinenko S.V. Modern possibilities of differential cytological diagnostics of proliferating mesothelium, mesothelioma and cancer metastases (literature review and results of own research). Klinicheskaya onkologiya 2015; 4(20).
- Gabris S., Kern L. Two color immunostaining of pleural effusions with Ber-EP4 and CK5/6. Cytopathology 2004; 15(Suppl 2): 14.
- Comin C.E., Saieva C., Messerini L. H-caldesmon, calretinin, estrogen receptor, and Ber-EP4: a useful combination of immunohistochemical markers for differentiating epithelioid peritoneal mesothelioma from serous papillary carcinoma of the ovary. Am J Surg Pathol 2007; 31(8): 1139–1148, https://doi.org/10.1097/pas.0b013e318033e7a8.
- Schnell U., Cirulli V., Giepmans B.N. EpCAM: structure and function in health and disease. Biochim Biophys Acta 2013; 1828(8): 1989–2001, https://doi.org/10.1016/j.bbamem.2013.04.018.
- Latza U., Niedobitek G., Schwarting R., Nekarda H., Stein H. Ber-EP4: new monoclonal antibody which distinguishes epithelia from mesothelial. J Clin Pathol 1990; 43(3): 213–219, https://doi.org/10.1136/jcp.43.3.213.
- Wang B., Li D., Ou X., Yi Q., Feng Y. Diagnostic accuracy of Ber-EP4 for metastatic adenocarcinoma in serous effusions: a meta-analysis. PLoS One 2014; 9(9): e107741, https://doi.org/10.1371/journal.pone.0107741.
- Maguire B., Whitaker D., Carrello S., Spagnolo D. Monoclonal antibody Ber-EP4: its use in the differential diagnosis of malignant mesothelioma and carcinoma in cell blocks of malignant effusions and FNA specimens. Diagn Cytopathol 1994; 10(2): 130–134, https://doi.org/10.1002/dc.2840100207.
- Volchenko N.N., Borisova O.V. Role of epithelial antigen Ber-EP4 in the study of exudates from serous sacs. Rossiyskiy onkologicheskiy zhurnal 2012; 2: 18–22.
- Ordóñez N.G. Value of the Ber-EP4 antibody in differentiating epithelial pleural mesothelioma from adenocarcinoma: the M.D. Anderson experience and a critical review of the literature. Am J Clin Pathol 1998; 109(1): 85–89, https://doi.org/10.1093/ajcp/109.1.85.
- Ordóñez N.G. The Immunohistochemical diagnosis of mesothelioma. Am J Surg Pathol 2003; 27(8): 1031–1051, https://doi.org/10.1097/00000478-200308000-00001.
- Morimoto A., Ito A., Hashimoto K., Nakano A., Nagasaka T., Yokoi T. New diagnostic technique for rapid fluorescence immunocytochemical staining of adenocarcinoma and mesothelial cells using liquid-based cytology. Acta Cytol 2014; 58(5): 461–468, https://doi.org/10.1159/000367706.
- Zinoviev S.V., Rachkov V.V., Utkin O.V., Savostikova M.V., Furminskaya E.Yu. A biochip for multiplex analysis and a method of studying cells in the diagnosis of oncological diseases. Patent WO 2017/204674 A1. 2017.









