Brain–Computer Interfaces for Upper Limb Motor Recovery after Stroke: Current Status and Development Prospects (Review)
Brain–computer interfaces (BCIs) are a group of technologies that allow mental training with feedback for post-stroke motor recovery. Varieties of these technologies have been studied in numerous clinical trials for more than 10 years, and their construct and software are constantly being improved. Despite the positive treatment results and the availability of registered medical devices, there are currently a number of problems for the wide clinical application of BCI technologies. This review provides information on the most studied types of BCIs and its training protocols and describes the evidence base for the effectiveness of BCIs for upper limb motor recovery after stroke. The main problems of scaling this technology and ways to solve them are also described.
Introduction
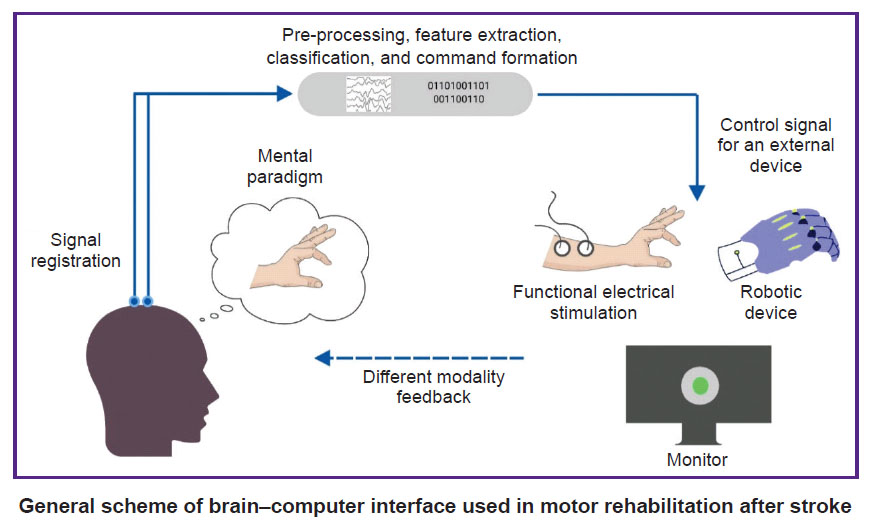
Brain–computer interface (BCI) is a technology that allows to convert data on the electrical or metabolic activity of the brain into control signals for an external technical device. In post-stroke rehabilitation, BCI is used to provide feedback to a patient during motor imagery training [1–3]. The scientific justification for this method has been the data on the positive effect of the motor imagery process on neuroplasticity due to activation of motor structures of the central nervous system (CNS) [4–8]. By providing feedback during motor imagery, the BCI systems enhance the effectiveness of such training sessions [9]. In general, training with the use of the BCI technology in patients after stroke includes the following processes: a patient is asked to mentally perform a movement of the paralyzed limb; the BCI technology using non-invasive sensors records brain signals accompanying the mental performance of the task; in real time, these signals are recognized and converted into a control command for an external device; the patient is provided with feedback on the quality of the mental task performance using the external device [10].
To date, at least 20 randomized controlled trials (RCTs) on the use of BCI for upper limb motor recovery after stroke are known worldwide, and 11 systematic reviews, 8 of which are accompanied by a meta-analysis, have been published on this topic between 2019 and 2023 [11–21]. Foreign and domestic manufacturers have developed several medical devices for use in clinical practice of post-stroke rehabilitation [22–25].
In Russia, clinical trials of BCI after stroke first began in 2011 at Research Center of Neurology (Moscow, Russia) [26, 27]. In a subsequent multicentre RCT, it was shown that a course of training with the BCI–exoskeleton complex improved the rehabilitation results of patients with focal brain damage in terms of hand motor recovery [28]. The proven technology was subsequently registered as a medical device and is currently used in a number of clinical centres [24, 29].
Despite the extensive evidence base and the availability of ready-made BCI technologies, there are currently some limitations to their widespread use in post-stroke rehabilitation, and further research and development is underway [30–37].
The aim of this review is to analyse scientific articles devoted to the study of the use of BCI technologies in post-stroke upper limb paresis, to outline the main problems and prospects for further development in this field.
Literature search methodology
Articles from peer-reviewed, full-text, open access scientific journals on the use of non-invasive BCIs for upper limb motor recovery after stroke were selected for analysis. The search query was formulated according to the rules of the MEDLINE bibliographic database: ((brain–computer[tiab] OR brain–machine[tiab] OR neural interfac*[tiab]) OR “Brain–Computer interfaces”[Mesh]) AND stroke[mh] AND (upper extremity[tiab] OR hand[tiab] OR arm[tiab]). Additionally, a literature search was conducted in the eLIBRARY.RU system using the key words “brain–computer interface”, “neurocomputer interface”, “neurointerface”. The date of the search was July 3, 2023.
Varieties of brain–computer interface systems and their application after stroke
All BCIs used in research or in the practice of post-stroke rehabilitation have distinctive features (see the Figure). The training protocols and BCI models studied in RCTs differ in the control paradigm of the interface, the type of signal recorded, the online signal processing algorithm, and the type of external technical device for providing feedback.
|
General scheme of brain–computer interface used in motor rehabilitation after stroke |
Control paradigm. Patients are typically tasked to imagine the movement, i.e., to mentally recreate the kinaesthetic sensation of a particular action in a limb without actually performing it [28, 38–45]. However, several studies have used a different paradigm — the intention to perform certain movements [46–48]. During the performance of this paradigm, in contrast to motor imagination, a patient tries to move the paralyzed limb, which is accompanied by a multiple increase in the electromyographic response compared to rest [13, 49]. In doing so, the main types of movement were clenching the hand into a fist and/or opening the hand and, less frequently, isolated or multijoint movements of the fingers, wrist, forearm, and upper arm [13].
Control signals. Most RCTs used BCIs based on electroencephalogram (EEG) recording [11, 17], and only one used near-infrared spectroscopy (NIRS) to record brain activity signals [43]. EEG–BCIs are the most accessible varieties of this technology. As a rule, the synchronization/desynchronization response of sensorimotor rhythm over the primary somatosensory and motor cortex areas, corresponding to the process of motor imagination, is used as the recorded signal in them. In NIRS–BCIs, the sources of brain activity can be several parameters: changes in the concentration of oxy-, deoxy-, or total haemoglobin at a depth of up to 4 cm from the head surface [50]. To apply NIRS–BCIs, unlike EEG–BCIs, there is no need to use electrode gel, and the patient’s movements during training do not lead to serious signal distortions. This technology is less available than EEG–BCI and is therefore unlikely to be suitable for widespread use. However, a portable NIRS–BCI system for home use has recently been proposed and tested on a small group of patients [51]. The application of this technology at home makes it possible to extend and prolong the rehabilitation program beyond the time-limited inpatient course.
Signal processing. Currently, there is no unified approach regarding signal processing algorithms in BCI systems. Many methods [52, 53] have been proposed and applied in various RCTs.
External technical devices. BCI algorithms convert brain signals into control commands for external technical devices that provide real-time feedback. An orthosis, robot, or exoskeleton arm in the BCI loop performs passive limb movement that the patient represents or attempts to perform. This kinaesthetic type of feedback has been used most often in previous RCTs, including in combination with visual feedback [28, 38, 39, 41, 45, 47, 48, 54]. In a number of studies, only visual feedback in the form of an abstract signal on a computer screen was used [43, 44]. Some authors consider the functional electrical stimulation (FES) in the BCI loop to be physiologically the most preferable. During FES, more motor and sensory axons are depolarized, more powerful signals from muscles spindles and Golgi tendon organs are delivered to the CNS, and pulses from the muscle spindles can activate motor neurons simultaneously with the descending cortical command when representing a movement, thus inducing Hebbian association [13, 55–58]. The efficacy of BCI with FES has also been studied in several RCTs [42, 46, 59–61].
Training courses. In the RCTs conducted, the frequency of BCI training sessions ranged from 2 [46] to 5 times a week [28, 45, 47, 54, 59, 60], and the total course duration ranged from 2 [28, 43] to 8 weeks [42], but most often was 4 weeks [38, 44, 45, 47, 59–61]. The total number of training sessions included from 6 [43] to 24 sessions [42], and the total training exposure ranged from 2 [43] to 27 h [39, 41].
Patients. The population of patients with ischemic or hemorrhagic stroke in the conducted RCTs was quite heterogeneous with respect to age, disease duration, lesion localization, and degree of motor deficit. The vast majority of RCTs were conducted in Asian countries, and the authors of a recent systematic review suggest it to be inappropriate to transfer the results of these studies to older European and North American populations of post-stroke patients [11].
Efficacy and safety of brain–computer interface technologies application after stroke
All published meta-analyses have found an advantage of BCI technologies over control groups with respect to upper limb motor function recovery after stroke as measured by Fugl-Meyer scale (see Appendix). As a rule, a medium effect size was observed, with standardized mean difference (SMD) or Hedges’ g scores greater than 0.5. The benefit of training with BCI has also been shown in terms of increased activity of daily living according to the modified Barthel index with a large effect size (SMD>1.0) [18, 20, 21].
Two studies conducted a meta-analysis in a subgroup of studies that included an additional follow-up period [14, 17]. An earlier study [14] found no effect in 6 weeks — 12 months after the end of the training course. In a more recent meta-analysis [17], which included a larger number of RCTs, the benefit of BCI over control groups persisted 2–36 weeks after the end of the study, but with a small effect size (SMD=0.33).
Besides, in studies evaluating recovery indices by functional magnetic resonance imaging (fMRI) or EEG, training with BCI has been shown to promote functional brain recovery with a large effect size (SMD=1.11; p<0.001) [15].
In all RCTs, no serious adverse events were reported. Some patients experienced headache, increased blood pressure, upper arm pain, skin hypersensitivity to electrode gel, and many patients experienced fatigue during training sessions. According to the meta-analysis [20], the incidence of adverse events and patient dropout rates were comparable in the BCI and control groups.
Factors influencing the efficacy of brain–computer interface technologies
In systematic reviews [14, 21], additional subgroup meta-analyses were performed to identify possible factors influencing the efficacy of BCI (see Appendix).
Two meta-analyses evaluated the dependence of BCI efficacy on the post-stroke time. The effect size in the subgroup of patients, which had a stroke less than 6 months ago (subacute phase), was higher than in the subgroup, the patients of which had a stroke 6 or more months ago (chronic phase) [16, 20]. However, no statistically significant differences in the BCI efficacy were found between groups with different post-stroke time.
The BCI with FES, compared to BCIs connected to robotic devices or with visual feedback only, turned out to be the most effective model of this technology, as shown in four meta-analyses [14, 17, 19, 20]. All of these studies have found a large effect size (SMD or Hedges’ g >1.0) when the use of FES–BCI was compared with the control group, which used FES without BCI control.
Attempting to make a movement may be a more favourable paradigm for controlling BCI than motor imagination. Two meta-analyses have shown a trend of greater effects of BCI training using the movement-attempt paradigm [14, 17]. However, due to the statistically insignificant differences in the effect between studies with different BCI control paradigms and considering the fact that the movement-attempt paradigm was used in only two RCTs, additional studies are needed to determine the influence of this factor more precisely.
Two meta-analyses additionally studied the possible influence of selected brain signal processing algorithms on the efficacy of the BCI technology. It has been shown that the use of spectral power in a single frequency band compared to the use of filters in several bands [17], as well as the use of sensorimotor rhythm control algorithms from leads located over motor cortical areas compared to the classification of EEG from numerous leads located over the entire surface of the head, are accompanied by a larger effect size [19].
Problems of widespread application of brain–computer interface technologies and ways to solve them
The widespread introduction of BCI technologies into clinical practice is currently hindered by a number of problems related to the technical features of existing BCI models, approaches to signal processing, and the current level of understanding the processes underlying motor recovery on the background of mental training [62–68].
One of the key challenges is the difference in individual human ability to control non-invasive BCIs using a motor imagery paradigm [69]. To master this skill, individuals usually require several BCI training sessions. However, even after training, the quality of control often remains low or instable, which demotivates patients. In addition, it has been shown that higher BCI control quality indicators are accompanied by higher motor recovery indicators [70]. At the same time, between 10 and 30% of users never achieve a proper level of BCI control. Some researchers call this phenomenon “BCI illiteracy”, while others, criticizing this term, refer to it as a “BCI inefficiency”, which can be overcome by using more efficient signal processing algorithms or sufficiently long operator training [62, 71, 72]. Most patients after stroke can control the BCI, but the quality and specificity of control depends on the degree of brain damage and neurological deficit [73, 74].
To solve the problem of the BCI control training, approaches of multiphase training of the BCI operator are being considered, where more brain signal-sensitive fMRI, transcranial electrical stimulation, or NIRS technologies are used in the first stages of motor imagery training [62, 75–77]. Developers continue to improve current signal processing approaches to increase the BCI control quality [78–84]. There is some hope for the application of deep learning algorithms in the BCI systems, including to overcome the phenomenon of “BCI illiteracy” and to ensure faster operator training [85–87]. It has also been shown that multimodal feedback (a combination of visual, auditory and somatosensory feedback) can improve the BCI control learning process [88, 89]. In cases where it is difficult for a patient to mentally imagine the movement, it is desirable to use the movement-attempt paradigm, which has been well established in some RCTs [46–48, 90].
Patient fatigue during BCI sessions is also a practical problem. Fatigue is a frequent symptom after stroke [91], and during the BCI control process it is necessary to concentrate attention for quite a long time, focusing on the mental task at hand. This problem can be overcome by providing breaks every 15 min of a training session [20], as well as by using more motivating and varied feedback in the form of a game [92, 93].
Besides, modern medical technologies should reduce the burden on health care workers and should be adapted for independent use by patients at home [94]. Most BCI developments to date do not meet these criteria. BCIs are cumbersome, require long sensor installation time and training to set up the system. Wireless high-impedance EEG systems with dry electrodes and an easy-to-operate system to launch the BCI on a mobile device can solve this problem [95–98].
With regard to the fundamental aspects of the application of rehabilitation BCIs based on motor imagery paradigm, the issue remains open as to which non-motor, non-specific mechanisms are involved in mental training-based motor recovery process. A high level of focusing on the task to control the BCI over an extended period of training may lead to an overall improvement in brain functioning, manifested by recovery of both motor and cognitive functions, which have not been adequately assessed in the majority of the RCTs conducted. Future research needs to determine whether motor learning on the background of the BCI training is a result of improvement in cognitive functions or whether the improvement in cognitive functions is secondary [62, 99, 100].
Conclusion
From the standpoint of evidence-based medicine, training using BCI is an effective method of upper limb motor function recovery after stroke. This is particularly true for FES–BCI technologies. In addition, training using BCI involves an active motor imagery or movement-attempt paradigm, being the only active rehabilitation method for patients with severe paresis or plegia. Currently, there are a number of challenges to scaling BCI technologies in clinical practice. However, considering the shortage of personnel for classical kinesiotherapy, innovative BCI technologies remain in demand, and further developments on their basis and technical improvement are sufficiently justified.
Authors’ contribution: O.A. Mokienko — collection, analysis, and compilation of literature data, writing the manuscript text, work with graphic materials; R.Kh. Lyukmanov — analysis and compilation of literature data, editing of the manuscript text; P.D. Bobrov — analysis and compilation of literature data, editing of the manuscript text; N.A. Suponeva — justification of the study concept, critical revision of the manuscript text; M.A. Piradov — justification of the study concept, critical revision of the manuscript text, generalization of the analysis results.
Study funding. The work was performed within the framework of the State assignments of the Ministry of Education and Science of the Russian Federation at the Federal State Budgetary Scientific Institution Research Center of Neurology and Institute of Higher Nervous Activity and Neurophysiology of Russian Academy of Science (Moscow, Russia).
There are no conflicts of interest.
References
- Khan M.A., Das R., Iversen H.K., Puthusserypady S. Review on motor imagery based BCI systems for upper limb post-stroke neurorehabilitation: from designing to application. Comput Biol Med 2020; 123: 103843, https://doi.org/10.1016/j.compbiomed.2020.103843.
- Khrulev A.E., Kuryatnikova K.M., Belova A.N., Popova P.S., Khrulev S.E. Modern rehabilitation technologies of patients with motor disorders at an early rehabilitation of stroke (review). Sovremennye tehnologii v medicine 2022; 14(6): 64, https://doi.org/10.17691/stm2022.14.6.07.
- Molinari M., Masciullo M. Stroke and potential benefits of brain-computer interface. Handb Clin Neurol 2020; 168: 25–32, https://doi.org/10.1016/b978-0-444-63934-9.00003-2.
- Mokienko O.A., Chernikova L.A., Frolov A.A., Bobrov P.D. Motor imagery and its practical application. Neurosci Behav Physi 2014; 44: 483–489, https://doi.org/10.1007/s11055-014-9937-y.
- Mokienko O.A., Chervyakov A.V., Kulikova S.N., Bobrov P.D., Chernikova L.A., Frolov A.A., Piradov M.A. Increased motor cortex excitability during motor imagery in brain-computer interface trained subjects. Front Comput Neurosci 2013; 7: 168, https://doi.org/10.3389/fncom.2013.00168.
- Girges C., Vijiaratnam N., Zrinzo L., Ekanayake J., Foltynie T. Volitional control of brain motor activity and its therapeutic potential. Neuromodulation 2022; 25(8): 1187–1196, https://doi.org/10.1016/j.neurom.2022.01.007.
- Bhagat N.A., Yozbatiran N., Sullivan J.L., Paranjape R., Losey C., Hernandez Z., Keser Z., Grossman R., Francisco G.E., O’Malley M.K., Contreras-Vidal J.L. Neural activity modulations and motor recovery following brain-exoskeleton interface mediated stroke rehabilitation. Neuroimage Clin 2020; 28: 102502, https://doi.org/10.1016/j.nicl.2020.102502.
- Yuan K., Chen C., Wang X., Chu W.C.W., Tong R.K.Y. BCI training effects on chronic stroke correlate with functional reorganization in motor-related regions: a concurrent EEG and fMRI study. Brain Sci 2021; 11(1): 56, https://doi.org/10.3390/brainsci11010056.
- Liao W., Li J., Zhang X., Li C. Motor imagery brain-computer interface rehabilitation system enhances upper limb performance and improves brain activity in stroke patients: a clinical study. Front Hum Neurosci 2023; 17: 1117670, https://doi.org/10.3389/fnhum.2023.1117670.
- Liu M., Ushiba J. Brain-machine interface (BMI)-based neurorehabilitation for post-stroke upper limb paralysis. Keio J Med 2022; 71(4): 82–92, https://doi.org/10.2302/kjm.2022-0002-oa.
- Carvalho R., Dias N., Cerqueira J.J. Brain-machine interface of upper limb recovery in stroke patients rehabilitation: a systematic review. Physiother Res Int 2019; 24(2): e1764, https://doi.org/10.1002/pri.1764.
- Baniqued P.D.E., Stanyer E.C., Awais M., Alazmani A., Jackson A.E., Mon-Williams M.A., Mushtaq F., Holt R.J. Brain-computer interface robotics for hand rehabilitation after stroke: a systematic review. J Neuroeng Rehabil 2021; 18(1): 15, https://doi.org/10.1186/s12984-021-00820-8.
- Fu J., Chen S., Jia J. Sensorimotor rhythm-based brain-computer interfaces for motor tasks used in hand upper extremity rehabilitation after stroke: a systematic review. Brain Sci 2022; 13(1): 56, https://doi.org/10.3390/brainsci13010056.
- Bai Z., Fong K.N.K., Zhang J.J., Chan J., Ting K.H. Immediate and long-term effects of BCI-based rehabilitation of the upper extremity after stroke: a systematic review and meta-analysis. J Neuroeng Rehabil 2020; 17(1): 57, https://doi.org/10.1186/s12984-020-00686-2.
- Kruse A., Suica Z., Taeymans J., Schuster-Amft C. Effect of brain-computer interface training based on non-invasive electroencephalography using motor imagery on functional recovery after stroke — a systematic review and meta-analysis. BMC Neurol 2020; 20(1): 385, https://doi.org/10.1186/s12883-020-01960-5.
- Yang W., Zhang X., Li Z., Zhang Q., Xue C., Huai Y. The effect of brain-computer interface training on rehabilitation of upper limb dysfunction after stroke: a meta-analysis of randomized controlled trials. Front Neurosci 2021; 15: 766879, https://doi.org/10.3389/fnins.2021.766879.
- Mansour S., Ang K.K., Nair K.P.S., Phua K.S., Arvaneh M. Efficacy of brain-computer interface and the impact of its design characteristics on poststroke upper-limb rehabilitation: a systematic review and meta-analysis of randomized controlled trials. Clin EEG Neurosci 2022; 53(1): 79–90, https://doi.org/10.1177/15500594211009065.
- Peng Y., Wang J., Liu Z., Zhong L., Wen X., Wang P., Gong X., Liu H. The application of brain-computer interface in upper limb dysfunction after stroke: a systematic review and meta-analysis of randomized controlled trials. Front Hum Neurosci 2022; 16: 798883, https://doi.org/10.3389/fnhum.2022.798883.
- Nojima I., Sugata H., Takeuchi H., Mima T. Brain-computer interface training based on brain activity can induce motor recovery in patients with stroke: a meta-analysis. Neurorehabil Neural Repair 2022; 36(2): 83–96, https://doi.org/10.1177/15459683211062895.
- Xie Y.L., Yang Y.X., Jiang H., Duan X.Y., Gu L.J., Qing W., Zhang B., Wang Y.X. Brain-machine interface-based training for improving upper extremity function after stroke: a meta-analysis of randomized controlled trials. Front Neurosci 2022; 16: 949575, https://doi.org/10.3389/fnins.2022.949575.
- Shou Y.Z., Wang X.H., Yang G.F. Verum versus Sham brain-computer interface on upper limb function recovery after stroke: a systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore) 2023; 102(26): e34148, https://doi.org/10.1097/md.0000000000034148.
- IpsiHand rehab device for stroke survivors. Neurolutions; 2023. URL: https://www.neurolutions.com/ipsihand.
- Bundy D.T., Souders L., Baranyai K., Leonard L., Schalk G., Coker R., Moran D.W., Huskey T., Leuthardt E.C. Contralesional brain–computer interface control of a powered exoskeleton for motor recovery in chronic stroke survivors. Stroke 2017; 48(7): 1908–1915, https://doi.org/10.1161/strokeaha.116.016304.
- Ekzokist’-2 [Exo-hand-2]. Ekzoplast; 2023. URL: https://exoplast.ru/.
- Ortez-1. Androidnaya tekhnika; 2023. URL: https://npo-at.com/production/orthosis/.
- Mokienko O.A., Lyukmanov R.Kh., Chernikova L.A., Suponeva N.A., Piradov M.A., Frolov A.A. Brain-computer interface: the first clinical experience in Russia. Hum Physiol 2016; 42(1): 24–31, https://doi.org/10.1134/s0362119716010126.
- Lyukmanov R.Kh., Aziatskaya G.A., Mokienko O.A., Varako N.A., Kovyazina M.S., Suponeva N.A., Chernikova L.A., Frolov A.A., Piradov M.A. Post-stroke rehabilitation training with a brain–computer interface: a clinical and neuropsychological study. Zhurnal nevrologii i psihiatrii im. S.S. Korsakova 2018; 118(8): 43–51, https://doi.org/10.17116/jnevro201811808143.
- Frolov A.A., Mokienko O., Lyukmanov R., Biryukova E., Kotov S., Turbina L., Nadareyshvily G., Bushkova Y. Post-stroke rehabilitation training with a motor-imagery-based brain-computer interface (BCI)-controlled hand exoskeleton: a randomized controlled multicenter trial. Front Neurosci 2017; 11: 400, https://doi.org/10.3389/fnins.2017.00400.
- Frolov A.A., Bobrov P.D., Biryukova E.V., Silchenko A.V., Kondur A.A., Dzhalagoniya I.Z., Massion J. Electrical, hemodynamic, and motor activity in BCI post-stroke rehabilitation: clinical case study. Front Neurol 2018; 9: 1135, https://doi.org/10.3389/fneur.2018.01135.
- Zhang R., Wang C., He S., Zhao C., Zhang K., Wang X., Li Y. An adaptive brain-computer interface to enhance motor recovery after stroke. IEEE Trans Neural Syst Rehabil Eng 2023; 31: 2268–2278, https://doi.org/10.1109/tnsre.2023.3272372.
- Fu J., Chen S., Shu X., Lin Y., Jiang Z., Wei D., Gao J., Jia J. Functional-oriented, portable brain-computer interface training for hand motor recovery after stroke: a randomized controlled study. Front Neurosci 2023; 17: 1146146, https://doi.org/10.3389/fnins.2023.1146146.
- Craik A., González-España J.J., Alamir A., Edquilang D., Wong S., Sánchez Rodríguez L., Feng J., Francisco G.E., Contreras-Vidal J.L. Design and validation of a low-cost mobile EEG-based brain-computer interface. Sensors (Basel) 2023; 23(13): 5930, https://doi.org/10.3390/s23135930.
- Gao Z., Pang Z., Chen Y., Lei G., Zhu S., Li G., Shen Y., Xu W. Restoring after central nervous system injuries: neural mechanisms and translational applications of motor recovery. Neurosci Bull 2022; 38(12): 1569–1587, https://doi.org/10.1007/s12264-022-00959-x.
- Behboodi A., Lee W.A., Hinchberger V.S., Damiano D.L. Determining optimal mobile neurofeedback methods for motor neurorehabilitation in children and adults with non-progressive neurological disorders: a scoping review. J Neuroeng Rehabil 2022; 19(1): 104, https://doi.org/10.1186/s12984-022-01081-9.
- Fu J., Jiang Z., Shu X., Chen S., Jia J. Correlation between the ERD in grasp/open tasks of BCIs and hand function of stroke patients: a cross-sectional study. Biomed Eng Online 2023; 22(1): 36, https://doi.org/10.1186/s12938-023-01091-1.
- Zanona A.F., Piscitelli D., Seixas V.M., Scipioni K.R.D.D.S., Bastos M.S.C., de Sá L.C.K., Monte-Silva K., Bolivar M., Solnik S., De Souza R.F. Brain-computer interface combined with mental practice and occupational therapy enhances upper limb motor recovery, activities of daily living, and participation in subacute stroke. Front Neurol 2022; 13: 1041978, https://doi.org/10.3389/fneur.2022.1041978.
- Gao W., Cui Z., Yu Y., Mao J., Xu J., Ji L., Kan X., Shen X., Li X., Zhu S., Hong Y. Application of a brain-computer interface system with visual and motor feedback in limb and brain functional rehabilitation after stroke: case report. Brain Sci 2022; 12(8): 1083, https://doi.org/10.3390/brainsci12081083.
- Ang K.K., Chua K.S.G., Phua K.S., Wang C., Chin Z.Y., Kuah C.W., Low W., Guan C. A randomized controlled trial of EEG-based motor imagery brain-computer interface robotic rehabilitation for stroke. Clin EEG Neurosci 2015; 46(4): 310–320, https://doi.org/10.1177/1550059414522229.
- Ang K.K., Guan C., Phua K.S., Wang C., Zhou L., Tang K.Y., Ephraim Joseph G.J., Kuah C.W.K., Chua K.S.G. Brain-computer interface-based robotic end effector system for wrist and hand rehabilitation: results of a three-armed randomized controlled trial for chronic stroke. Front Neuroeng 2014; 7: 30, https://doi.org/10.3389/fneng.2014.00030.
- Ang K.K., Guan C., Phua K.S., Wang C., Zhao L., Teo W.P., Chen C., Ng Y.S., Chew E. Facilitating effects of transcranial direct current stimulation on motor imagery brain-computer interface with robotic feedback for stroke rehabilitation. Arch Phys Med Rehabil 2015; 96(3 Suppl): S79–S87, https://doi.org/10.1016/j.apmr.2014.08.008.
- Cheng N., Phua K.S., Lai H.S., Tam P.K., Tang K.Y., Cheng K.K., Yeow R.C., Ang K.K., Guan C., Lim J.H. Brain-computer interface-based soft robotic glove rehabilitation for stroke. IEEE Trans Biomed Eng 2020; 67(12): 3339–3351, https://doi.org/10.1109/tbme.2020.2984003.
- Li M., Liu Y., Wu Y., Liu S., Jia J., Zhang L. Neurophysiological substrates of stroke patients with motor imagery-based brain-computer interface training. Int J Neurosci 2014; 124(6): 403–415, https://doi.org/10.3109/00207454.2013.850082.
- Mihara M., Hattori N., Hatakenaka M., Yagura H., Kawano T., Hino T., Miyai I. Near-infrared spectroscopy-mediated neurofeedback enhances efficacy of motor imagery-based training in poststroke victims: a pilot study. Stroke 2013; 44(4): 1091–1098, https://doi.org/10.1161/strokeaha.111.674507.
- Pichiorri F., Morone G., Petti M., Toppi J., Pisotta I., Molinari M., Paolucci S., Inghilleri M., Astolfi L., Cincotti F., Mattia D. Brain-computer interface boosts motor imagery practice during stroke recovery. Ann Neurol 2015; 77(5): 851–865, https://doi.org/10.1002/ana.24390.
- Wu Q., Yue Z., Ge Y., Ma D., Yin H., Zhao H., Liu G., Wang J., Dou W., Pan Y. Brain functional networks study of subacute stroke patients with upper limb dysfunction after comprehensive rehabilitation including BCI training. Front Neurol 2019; 10: 1419, https://doi.org/10.3389/fneur.2019.01419.
- Biasiucci A., Leeb R., Iturrate I., Perdikis S., Al-Khodairy A., Corbet T., Schnider A., Schmidlin T., Zhang H., Bassolino M., Viceic D., Vuadens P., Guggisberg A.G., Millán J.D.R. Brain-actuated functional electrical stimulation elicits lasting arm motor recovery after stroke. Nat Commun 2018; 9(1): 2421, https://doi.org/10.1038/s41467-018-04673-z.
- Ramos-Murguialday A., Broetz D., Rea M., Läer L., Yilmaz O., Brasil F.L., Liberati G., Curado M.R., Garcia-Cossio E., Vyziotis A., Cho W., Agostini M., Soares E., Soekadar S., Caria A., Cohen L.G., Birbaumer N. Brain-machine interface in chronic stroke rehabilitation: a controlled study. Ann Neurol 2013; 74(1): 100–108, https://doi.org/10.1002/ana.23879.
- Chen S., Cao L., Shu X., Wang H., Ding L., Wang S.H., Jia J. Longitudinal electroencephalography analysis in subacute stroke patients during intervention of brain-computer interface with exoskeleton feedback. Front Neurosci 2020; 14: 809, https://doi.org/10.3389/fnins.2020.00809.
- Antelis J.M., Montesano L., Ramos-Murguialday A., Birbaumer N., Minguez J. Decoding upper limb movement attempt from EEG measurements of the contralesional motor cortex in chronic stroke patients. IEEE Trans Biomed Eng 2017; 64(1): 99–111, https://doi.org/10.1109/tbme.2016.2541084.
- Soekadar S.R., Kohl S.H., Mihara M., von Lühmann A. Optical brain imaging and its application to neurofeedback. Neuroimage Clin 2021; 30: 102577, https://doi.org/10.1016/j.nicl.2021.102577.
- Lee Friesen C., Lawrence M., Ingram T.G.J., Boe S.G. Home-based portable fNIRS-derived cortical laterality correlates with impairment and function in chronic stroke. Front Hum Neurosci 2022; 16: 1023246, https://doi.org/10.3389/fnhum.2022.1023246.
- Hramov A.E., Maksimenko V.A., Pisarchik A.N. Physical principles of brain–computer interfaces and their applications for rehabilitation, robotics and control of human brain states. Phys Rep 2021; 918: 1–133, https://doi.org/10.1016/j.physrep.2021.03.002.
- Lotte F., Bougrain L., Cichocki A., Clerc M., Congedo M., Rakotomamonjy A., Yger F. A review of classification algorithms for EEG-based brain-computer interfaces: a 10 year update. J Neural Eng 2018; 15(3): 031005, https://doi.org/10.1088/1741-2552/aab2f2.
- Wang X., Wong W.W., Sun R., Chu W.C.W., Tong K.Y. Differentiated effects of robot hand training with and without neural guidance on neuroplasticity patterns in chronic stroke. Front Neurol 2018; 9: 810, https://doi.org/10.3389/fneur.2018.00810.
- Reynolds C., Osuagwu B.A., Vuckovic A. Influence of motor imagination on cortical activation during functional electrical stimulation. Clin Neurophysiol 2015; 126(7): 1360–1369, https://doi.org/10.1016/j.clinph.2014.10.007.
- Bergquist A.J., Clair J.M., Lagerquist O., Mang C.S., Okuma Y., Collins D.F. Neuromuscular electrical stimulation: implications of the electrically evoked sensory volley. Eur J Appl Physiol 2011; 111(10): 2409–2426, https://doi.org/10.1007/s00421-011-2087-9.
- Chen L., Gu B., Wang Z., Zhang L., Xu M., Liu S., He F., Ming D. EEG-controlled functional electrical stimulation rehabilitation for chronic stroke: system design and clinical application. Front Med 2021; 15(5): 740–749, https://doi.org/10.1007/s11684-020-0794-5.
- Sinha A.M., Nair V.A., Prabhakaran V. Brain-computer interface training with functional electrical stimulation: facilitating changes in interhemispheric functional connectivity and motor outcomes post-stroke. Front Neurosci 2021; 15: 670953, https://doi.org/10.3389/fnins.2021.670953.
- Lee S.H., Kim S.S., Lee B.H. Action observation training and brain-computer interface controlled functional electrical stimulation enhance upper extremity performance and cortical activation in patients with stroke: a randomized controlled trial. Physiother Theory Pract 2022; 38(9): 1126–1134, https://doi.org/10.1080/09593985.2020.1831114.
- Kim T., Kim S., Lee B. Effects of action observational training plus brain-computer interface-based functional electrical stimulation on paretic arm motor recovery in patient with stroke: a randomized controlled trial. Occup Ther Int 2016; 23(1): 39–47, https://doi.org/10.1002/oti.1403.
- Miao Y., Chen S., Zhang X., Jin J., Xu R., Daly I., Jia J., Wang X., Cichocki A., Jung T.P. BCI-based rehabilitation on the stroke in sequela stage. Neural Plast 2020; 2020: 8882764, https://doi.org/10.1155/2020/8882764.
- Simon C., Bolton D.A.E., Kennedy N.C., Soekadar S.R., Ruddy K.L. Challenges and opportunities for the future of brain-computer interface in neurorehabilitation. Front Neurosci 2021; 15: 699428, https://doi.org/10.3389/fnins.2021.699428.
- Colucci A., Vermehren M., Cavallo A., Angerhöfer C., Peekhaus N., Zollo L., Kim W.S., Paik N.J., Soekadar S.R. Brain-computer interface-controlled exoskeletons in clinical neurorehabilitation: ready or not? Neurorehabil Neural Repair 2022; 36(12): 747–756, https://doi.org/10.1177/15459683221138751.
- Mridha M.F., Das S.C., Kabir M.M., Lima A.A., Islam M.R., Watanobe Y. Brain-computer interface: advancement and challenges. Sensors (Basel) 2021; 21(17): 5746, https://doi.org/10.3390/s21175746.
- Jervis-Rademeyer H., Ong K., Djuric A., Munce S., Musselman K.E., Marquez-Chin C. Therapists’ perspectives on using brain-computer interface-triggered functional electrical stimulation therapy for individuals living with upper extremity paralysis: a qualitative case series study. J Neuroeng Rehabil 2022; 19(1): 127, https://doi.org/10.1186/s12984-022-01107-2.
- Padfield N., Zabalza J., Zhao H., Masero V., Ren J. EEG-based brain-computer interfaces using motor-imagery: techniques and challenges. Sensors (Basel) 2019; 19(6): 1423, https://doi.org/10.3390/s19061423.
- Saha S., Mamun K.A., Ahmed K., Mostafa R., Naik G.R., Darvishi S., Khandoker A.H., Baumert M. Progress in brain computer interface: challenges and opportunities. Front Syst Neurosci 2021; 15: 578875, https://doi.org/10.3389/fnsys.2021.578875.
- Angerhöfer C., Colucci A., Vermehren M., Hömberg V., Soekadar S.R. Post-stroke rehabilitation of severe upper limb paresis in Germany — toward long-term treatment with brain-computer interfaces. Front Neurol 2021; 12: 772199, https://doi.org/10.3389/fneur.2021.772199.
- Bobrova E.V., Reshetnikova V.V., Vershinina E.A., Grishin A.A., Bobrov P.D., Frolov A.A., Gerasimenko Y.P. Success of hand movement imagination depends on personality traits, brain asymmetry, and degree of handedness. Brain Sci 2021; 11(7): 853, https://doi.org/10.3390/brainsci11070853.
- Sebastián-Romagosa M., Cho W., Ortner R., Murovec N., Von Oertzen T., Kamada K., Allison B.Z., Guger C. Brain computer interface treatment for motor rehabilitation of upper extremity of stroke patients — a feasibility study. Front Neurosci 2020; 14: 591435, https://doi.org/10.3389/fnins.2020.591435.
- Thompson M.C. Critiquing the concept of BCI illiteracy. Sci Eng Ethics 2019; 25(4): 1217–1233, https://doi.org/10.1007/s11948-018-0061-1.
- Wang T., Du S., Dong E. A novel method to reduce the motor imagery BCI illiteracy. Med Biol Eng Comput 2021; 59(11–12): 2205–2217, https://doi.org/10.1007/s11517-021-02449-0.
- Mansour S., Giles J., Ang K.K., Nair K.P.S., Phua K.S., Arvaneh M. Exploring the ability of stroke survivors in using the contralesional hemisphere to control a brain-computer interface. Sci Rep 2022; 12(1): 16223, https://doi.org/10.1038/s41598-022-20345-x.
- Chen S., Shu X., Jia J., Wang H., Ding L., He Z., Brauer S., Zhu X. Relation between sensorimotor rhythm during motor attempt/imagery and upper-limb motor impairment in stroke. Clin EEG Neurosci 2022; 53(3): 238–247, https://doi.org/10.1177/15500594211019917.
- Leamy D.J., Collins R., Ward T.E. Combining fNIRS and EEG to improve motor cortex activity classification during an imagined movement-based task. In: Foundations of augmented cognition. Directing the future of adaptive systems. Schmorrow D.D., Fidopiastis C.M. (editors). Springer Berlin Heidelberg; 2011; p. 177–185.
- Fazli S., Mehnert J., Steinbrink J., Curio G., Villringer A., Müller K.R., Blankertz B. Enhanced performance by a hybrid NIRS–EEG brain computer interface. Neuroimage 2012; 59(1): 519–529, https://doi.org/10.1016/j.neuroimage.2011.07.084.
- Liang W.D., Xu Y., Schmidt J., Zhang L.X., Ruddy K.L. Upregulating excitability of corticospinal pathways in stroke patients using TMS neurofeedback; a pilot study. Neuroimage Clin 2020; 28: 102465, https://doi.org/10.1016/j.nicl.2020.102465.
- de Seta V., Toppi J., Colamarino E., Molle R., Castellani F., Cincotti F., Mattia D., Pichiorri F. Cortico-muscular coupling to control a hybrid brain-computer interface for upper limb motor rehabilitation: a pseudo-online study on stroke patients. Front Hum Neurosci 2022; 16: 1016862, https://doi.org/10.3389/fnhum.2022.1016862.
- Al-Qazzaz N.K., Aldoori A.A., Ali S.H.B.M., Ahmad S.A., Mohammed A.K., Mohyee M.I. EEG signal complexity measurements to enhance BCI-based stroke patients’ rehabilitation. Sensors (Basel) 2023; 23(8): 3889, https://doi.org/10.3390/s23083889.
- Zhang R., Chen Y., Xu Z., Zhang L., Hu Y., Chen M. Recognition of single upper limb motor imagery tasks from EEG using multi-branch fusion convolutional neural network. Front Neurosci 2023; 17: 1129049, https://doi.org/10.3389/fnins.2023.1129049.
- Delisle-Rodriguez D., Silva L., Bastos-Filho T. EEG changes during passive movements improve the motor imagery feature extraction in BCIs-based sensory feedback calibration. J Neural Eng 2023; 20(1): 016047, https://doi.org/10.1088/1741-2552/acb73b.
- Wu D., Jiang X., Peng R. Transfer learning for motor imagery based brain-computer interfaces: a tutorial. Neural Netw 2022; 153: 235–253, https://doi.org/10.1016/j.neunet.2022.06.008.
- Varsehi H., Firoozabadi S.M.P. An EEG channel selection method for motor imagery based brain-computer interface and neurofeedback using Granger causality. Neural Netw 2021; 133: 193–206, https://doi.org/10.1016/j.neunet.2020.11.002.
- Al-Qazzaz N.K., Alyasseri Z.A.A., Abdulkareem K.H., Ali N.S., Al-Mhiqani M.N., Guger C. EEG feature fusion for motor imagery: a new robust framework towards stroke patients rehabilitation. Comput Biol Med 2021; 137: 104799, https://doi.org/10.1016/j.compbiomed.2021.104799.
- Zhang X., Ma Z., Zheng H., Li T., Chen K., Wang X., Liu C., Xu L., Wu X., Lin D., Lin H. The combination of brain-computer interfaces and artificial intelligence: applications and challenges. Ann Transl Med 2020; 8(11): 712, https://doi.org/10.21037/atm.2019.11.109.
- Cao L., Wu H., Chen S., Dong Y., Zhu C., Jia J., Fan C. A novel deep learning method based on an overlapping time window strategy for brain-computer interface-based stroke rehabilitation. Brain Sci 2022; 12(11): 1502, https://doi.org/10.3390/brainsci12111502.
- Hossain K.M., Islam M.A., Hossain S., Nijholt A., Ahad M.A.R. Status of deep learning for EEG-based brain-computer interface applications. Front Comput Neurosci 2022; 16: 1006763, https://doi.org/10.3389/fncom.2022.1006763.
- Sollfrank T., Ramsay A., Perdikis S., Williamson J., Murray-Smith R., Leeb R., Millán J.D.R., Kübler A. The effect of multimodal and enriched feedback on SMR-BCI performance. Clin Neurophysiol 2016; 127(1): 490–498, https://doi.org/10.1016/j.clinph.2015.06.004.
- Ma Z.Z., Wu J.J., Hua X.Y., Zheng M.X., Xing X.X., Ma J., Shan C.L., Xu J.G. Evidence of neuroplasticity with brain-computer interface in a randomized trial for post-stroke rehabilitation: a graph-theoretic study of subnetwork analysis. Front Neurol 2023; 14: 1135466, https://doi.org/10.3389/fneur.2023.1135466.
- Chen S., Shu X., Wang H., Ding L., Fu J., Jia J. The differences between motor attempt and motor imagery in brain-computer interface accuracy and event-related desynchronization of patients with hemiplegia. Front Neurorobot 2021; 15: 706630, https://doi.org/10.3389/fnbot.2021.706630.
- Alghamdi I., Ariti C., Williams A., Wood E., Hewitt J. Prevalence of fatigue after stroke: a systematic review and meta-analysis. Eur Stroke J 2021; 6(4): 319–332, https://doi.org/10.1177/23969873211047681.
- de Castro-Cros M., Sebastian-Romagosa M., Rodríguez-Serrano J., Opisso E., Ochoa M., Ortner R., Guger C., Tost D. Effects of gamification in BCI functional rehabilitation. Front Neurosci 2020; 14: 882, https://doi.org/10.3389/fnins.2020.00882.
- Ziadeh H., Gulyas D., Nielsen LD., Lehmann S., Nielsen T.B., Kjeldsen T.K.K., Hougaard B.I., Jochumsen M., Knoche H. “Mine works better”: examining the influence of embodiment in virtual reality on the sense of agency during a binary motor imagery task with a brain-computer interface. Front Psychol 2021; 12: 806424, https://doi.org/10.3389/fpsyg.2021.806424.
- Zulauf-Czaja A., Al-Taleb M.K.H., Purcell M., Petric-Gray N., Cloughley J., Vuckovic A. On the way home: a BCI-FES hand therapy self-managed by sub-acute SCI participants and their caregivers: a usability study. J Neuroeng Rehabil 2021; 18(1): 44, https://doi.org/10.1186/s12984-021-00838-y.
- McWilliams E.C., Barbey F.M., Dyer J.F., Islam M.N., McGuinness B., Murphy B., Nolan H., Passmore P., Rueda-Delgado L.M., Buick A.R. Feasibility of repeated assessment of cognitive function in older adults using a wireless, mobile, dry-EEG headset and tablet-based games. Front Psychiatry 2021; 12: 574482, https://doi.org/10.3389/fpsyt.2021.574482.
- Jamil N., Belkacem A.N., Ouhbi S., Lakas A. Noninvasive electroencephalography equipment for assistive, adaptive, and rehabilitative brain-computer interfaces: a systematic literature review. Sensors (Basel) 2021; 21(14): 4754, https://doi.org/10.3390/s21144754.
- Yang S., Li R., Li H., Xu K., Shi Y., Wang Q., Yang T., Sun X. Exploring the use of brain-computer interfaces in stroke neurorehabilitation. BioMed Res Int 2021; 2021: 9967348, https://doi.org/10.1155/2021/9967348.
- Hashimoto Y., Kakui T., Ushiba J., Liu M., Kamada K., Ota T. Portable rehabilitation system with brain-computer interface for inpatients with acute and subacute stroke: a feasibility study. Assist Technol 2022; 34(4): 402–410, https://doi.org/10.1080/10400435.2020.1836067.
- Borisova V.A., Isakova E.V., Kotov S.V. Possibilities of the brain–computer interface in the correction of post-stroke cognitive impairments. Zhurnal nevrologii i psihiatrii im. S.S. Korsakova 2022; 122(12-2): 60–66, https://doi.org/10.17116/jnevro202212212260.
- Liu X., Zhang W., Li W., Zhang S., Lv P., Yin Y. Effects of motor imagery based brain-computer interface on upper limb function and attention in stroke patients with hemiplegia: a randomized controlled trial. BMC Neurol 2023; 23(1): 136, https://doi.org/10.1186/s12883-023-03150-5.








