Structuring Characteristics of Biological Fluids of Patients with Combined Cardiovascular and Gastrointestinal Pathology
The aim of the investigation was a comparative study of the result of self- and initiated crystallization of saliva and urine in patients with an isolated ulcer disease, coronary heart disease (CHD), and the combination of both.
Materials and Methods. We studied saliva and urine samplings in 35 patients with isolated CHD, in 48 — with ulcer disease, and in 112 — with the combination of both. CHD was diagnosed based on a clinical study, as well as according to the findings of instrumental studies (ECG recording at rest and physical load, Holter ECG monitoring, echocardiography). The diagnosis of ulcer disease was verified by fibrogastroduodenoscopy; helicobacteriosis was revealed by biopsy and serologic testing. The characteristics of self- and initiated crystallization of biological substrates were assessed using a semiquantitative analysis. Normal saline was a basic substance for teziography.
Results. A combined pathology was found to have a specific character in the formation of crystallogenic properties of biological fluid facies of patients. This fact is consistent with the data indicating dysmetabolic disorders, which integrate the diseases under study and are caused by Helicobacter pylori. The findings both confirm the presence of metabolic response of the body on comorbidity and also can serve as the basis for the development of noninvasive technologies to monitor the effectiveness of Helicobacter pylori eradication.
Digestive and cardiovascular diseases take a significant position in the total morbidity pattern [1–5], the interaction between gastrointestinal (GI) tract and cardiovascular system being of special interest [2–4, 6–9]. So, GI pathology can result in functional disorders of cardiovascular system occurring indirectly through autonomic nervous system (ANS) [7]. On the other hand, ANS dysfunction can be caused by GI diseases, in particular, hypertonia of parasympathetic nervous system has been described to coincide with exacerbations of chronic medical diseases [7–9].
It should be noted that if the pathogenesis of isolated coronary heart disease (CHD) and ulcerative ulcer disease (UD) is thoroughly studied, the mechanisms of their combined action is still debatable [1–3, 7–9]. The discovery of metabolic changes accompanying this combined pathology will be of help in solving the problem [10–14]. According to current concepts, metabolic changes can be assessed using biocrystallomics [10, 15, 16].
The aim of the investigation was a comparative study of the result of self- and initiated crystallization of saliva and urine in patients with an isolated ulcer disease, coronary heart disease, and the combination of both.
Materials and Methods. We examined saliva and urine samples in 35 patients with isolated CHD, in 48 patients — with UD, and in 112 — with the combination of both. CHD was diagnosed based on a clinical study and the findings of instrumental studies (ECG recording at rest and physical load, Holter ECG monitoring, echocardiography). Functional class (FC) I angina was diagnosed in 45 patients (40.2%), FC II angina — in 67 (59.8%). The duration of CHD history varied from 2 to 8 years. 29 patients (25.8%) had in their past histories old (over 2 years) myocardial infarction. During the examination UD in remission was found in 94 patients (83.9%), UD exacerbations — in 18 patients (16.1%). FC I cardiac failure (Heart Failure Association, Russia, 2001) was revealed in 67 patients (59.8%), FC II — in 45 (40.2%).
The diagnosis of ulcer disease was verified by fibrogastroduodenoscopy. Duodenal ulcer was confirmed in 83 patients (74.1%), gastric ulcer — in 29 patients (25.9%). Helicobacteriosis was revealed using biopsy and serologic testing.
The study complies with the declaration of Helsinki (adopted in June, 1964 (Helsinki, Finland) and revised in October, 2000 (Edinburg, Scotland)) and approved by the Ethics Committee of Kirov State Medical Academy. Written informed consent was obtained from all patients.
The characteristics of self- and initiated crystallization of biological substrates were assessed using a semiquantitative analysis [15, 16]. Normal saline was a basic substance for teziography.
The results were processed using Statistica 6.0.
Results and Discussion. The examinations showed that the changes of crystallogenic activity of saliva and urine in this combined pathology have common features. So, the study of urine free crystal formation in patients with combined CHD and UD demonstrated that in fascies of all micropreparations there are both the substance with amorphous structure and a dendritic component, and we can visualize crystals of single crystal and dendritic rows (Fig. 1).
 Fig. 1. Urine crystalloscopy of an apparently healthy subject (а) and a patient with combination of CHD and gastric ulcer (b) Fig. 1. Urine crystalloscopy of an apparently healthy subject (а) and a patient with combination of CHD and gastric ulcer (b)
|
Marginal protein layer on these samples is not well-defined or can be visualized not along the entire length of facies. The assessment of facies destruction degree showing the sequence of crystallogenesis demonstrated numerous destroyed crystal structures. The findings were confirmed by visuametric analysis of crystalloscopic facies of the analyzed biological fluids of healthy subjects and patients with combined pathology (Fig. 2).
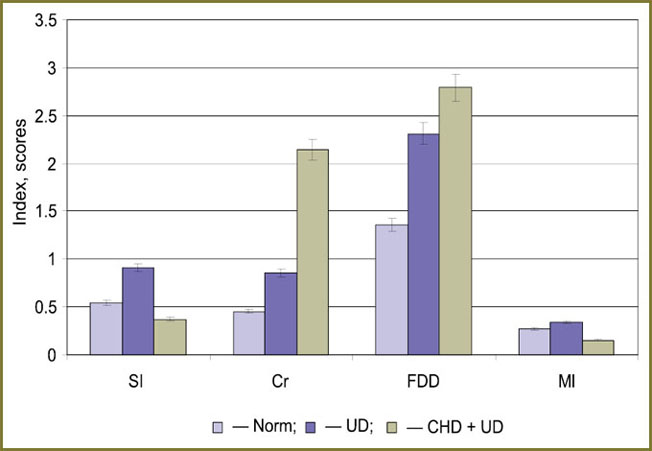 Fig. 2. Results of visuametric analysis of crystalloscopic urine facies in health, in isolated ulcer disease and in its combination with CHD. SI — structuredness index; Cr — crystallizability; FDD — facies destruction degree; Ml — marginal layer intensity Fig. 2. Results of visuametric analysis of crystalloscopic urine facies in health, in isolated ulcer disease and in its combination with CHD. SI — structuredness index; Cr — crystallizability; FDD — facies destruction degree; Ml — marginal layer intensity
|
Morphometric research of urine crystallograms showed facies in patients with gastric ulcer alone to be characterized by increased crystallogenic potential compared to biofluids of apparently healthy subjects.This is evident from the increase of structuredness index of the sample indicating complexity of structural construction, as well as crystallizability index showing biosubstrate quantitative crystallogenesis (density of crystals in a sample). Pathological character of this crystalloscopic “pattern” is emphasized by a high destruction level of structural elements.
When combined pathology is formed, the transformation of urine crystalloscopic facies has radically different features: in this case facies is formed by numerous single crystal elements with extremely high destruction degree as evidenced by corresponding indices of structuredness and crystallizability. A marginal layer of dried urine micropreparations in this group of patients can be hardly defined that is indicated by “setting to zero” of the parameter.
The study of free crystal formation of saliva with combined CHD and UD enabled to find out the following common factors: discrete part of all samples was represented by amorphous bodies and single crystal elements, extremely high density of crystallization centers in samples calling special attention (Fig. 3). There were numerous destroyed and changed structures. A marginal layer is intense along the entire perimeter of a micropreparation.
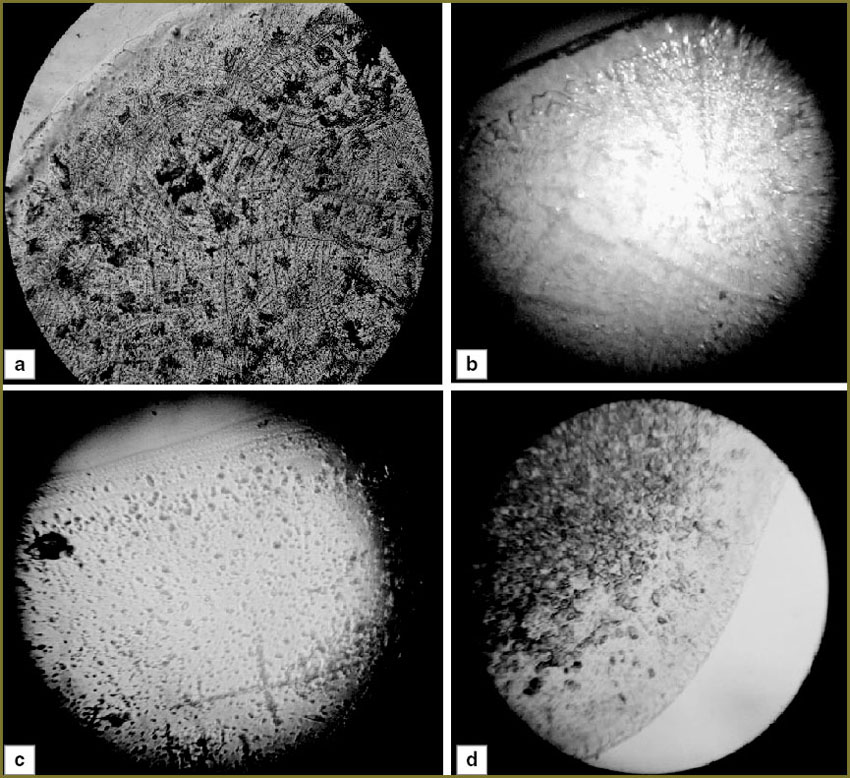 Fig. 3. Examples of oral crystalloscopic facies of: а — apparently healthy subjects; b — patients with isolated CHD; c — patients with isolated ulcer disease; d — patients with combined pathology of cardiovascular system and middle part of gastrointestinal tract Fig. 3. Examples of oral crystalloscopic facies of: а — apparently healthy subjects; b — patients with isolated CHD; c — patients with isolated ulcer disease; d — patients with combined pathology of cardiovascular system and middle part of gastrointestinal tract
|
The carried out visuametric analysis of crystalloscopic facies of saliva in combined pathology also demonstrated the formation of a new pathological “pattern”, which differs greatly from that typical for isolated diseases, and is not their algebraic mean (Fig. 4).
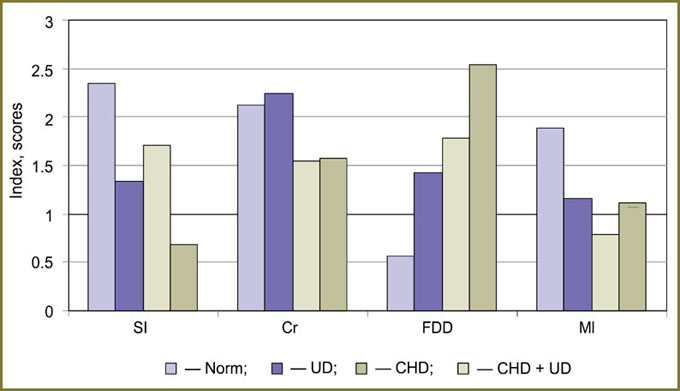 Fig. 4. Visuametry of oral fluid facies of apparently healthy subjects and patients with isolated and combined pathology of cardiovascular system and a middle part of gastrointestinal tract. Conventional symbols are shown in Fig. 2 Fig. 4. Visuametry of oral fluid facies of apparently healthy subjects and patients with isolated and combined pathology of cardiovascular system and a middle part of gastrointestinal tract. Conventional symbols are shown in Fig. 2
|
Transformation of crystalloscopic pattern of mixed saliva in patients with gastric ulcer alone was found to include moderate inhibition of structure formation appearing in growing number of single crystal elements in facies as indicated by evident decrease of SI level combined with minimum crystallizability increase. In case of CHD alone, there was moderate decrease of saliva crystallizability together with similar, though of less (in modulus) change of biofluid SI in relation to patients with isolated gastric ulcer. It should be noted that destruction of elements in dried oral samples of this group of patients was more intense than in gastroduodenal ulcerogenesis alone. Moreover, the patients of this group were found to have a marginal layer minimum in diameter.
The most significant alterations of oral crystal formation were found in patients with combined CHD and gastric ulcer. The crystallograms of these patients were characterized by the evident predominance of single crystal elements over dendritic ones, total density of the structures in facies being significantly reduced compared to both healthy subjects and the patients of other groups. The intensity of metabolic disorders in oral cavity of patients with combined pathology also indicated by subtotal destruction of facies structural elements.
Concurrently we carried out a comparative analysis of induced urine crystal formation in the patients under study (Fig. 5). Normalsalinewasusedasaninitiatingsolution. In combined pathology the initiation activity of the biological fluid under study was found to change significantly as well, it being manifested by the enlargement of structural elements and total density reduction of crystals and a high destruction degree.
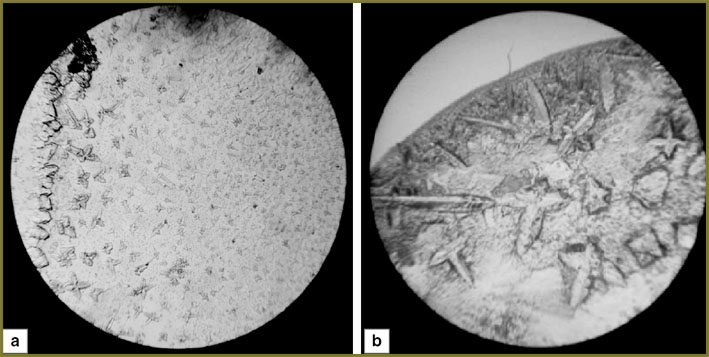 Fig. 5. Urine teziography of an apparently healthy subject (а) and a patient with combined CHD and gastric ulcer (b); basic substance — normal saline Fig. 5. Urine teziography of an apparently healthy subject (а) and a patient with combined CHD and gastric ulcer (b); basic substance — normal saline
|
Comparative morphometric analysis of crystallogenic activity of urine samples suggested the similar changes of induced crystallogenesis in both isolated gastric ulcer and in its combination with CHD (Fig. 6). In particular, due to significant tendency for the increase in size of single crystal and dendritic elements of facies we observed significant decrease of teziographic index.However, isolated and combined pathologies are essentially different in the parameter of crystallinity, which is similar to crystallogram SI: if a patient has only gastric ulcer, facies is almost completely formed by few single crystals, while in dehydrated urine samples of patients with combined pathology ramified dendritic elements prevail, monocrystals being a minimum part of a sample. Potential presence of intense imbalance of protein component in urine samples results in nearly total disappearance of a marginal layer of facies in patients with coronary heart disease and gastric ulcer.
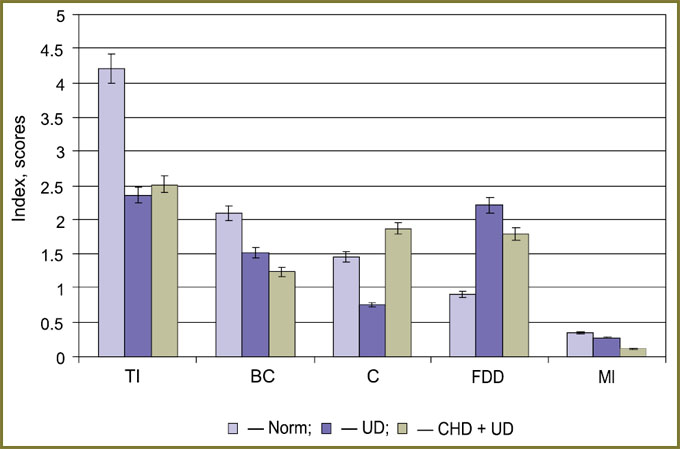 Fig. 6. Visuametric analysis findings of urine teziograms in health and in isolated and combined CHD and gastric ulcer. Conventional symbols — see Fig. 2, TI — teziographic index; BC — belt coefficient; C — crystallinity Fig. 6. Visuametric analysis findings of urine teziograms in health and in isolated and combined CHD and gastric ulcer. Conventional symbols — see Fig. 2, TI — teziographic index; BC — belt coefficient; C — crystallinity
|
Teziographic assessment of patients` saliva enabled to reveal the following: the number of crystallization centers in a test sample (“biofluid–basic substance” system) significantly exceeds the number of those in a control one (facies formed by basic substance). Among discrete constituents of facies there prevailed crystal elements, though there was also an amorphous component (Fig. 7). A marginal layer was evident along the entire facies length that indicates the significant amount of protein component in the samples.
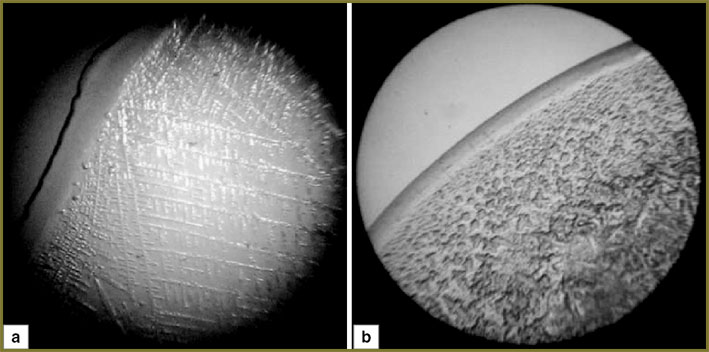 Fig. 7. Saliva teziography of an apparently healthy subject (а) and a patient with combined CHD and gastric ulcer (b); basic substance — normal saline Fig. 7. Saliva teziography of an apparently healthy subject (а) and a patient with combined CHD and gastric ulcer (b); basic substance — normal saline
|
Visuametric analysis of oral fluid facies of apparently healthy subjects and patients with isolated and combined pathology of cardiovascular system and a middle part of GI tract clearly demonstrated the uniqueness of the alteration of crystallogenic properties of this biosubstrate in this combination of the disease (Fig. 8). So, the teziograms of mixed saliva of patients with gastric ulcer are characterized by “simplified” structure construction of elements with their density increase, for CHD patients — minimum growth of the number of dendritic crystals, without significant increase of total initiation potential of biological fluid — teziographic index; while in combined pathology there were observed both: the reduction of nitiation potential of biosubstrate, and dramatic change of the prevailing type of structural elements: from dendritic elements (prevailing in health) to amorphous elements, they occupying nearly the entire space of a micropreparation.
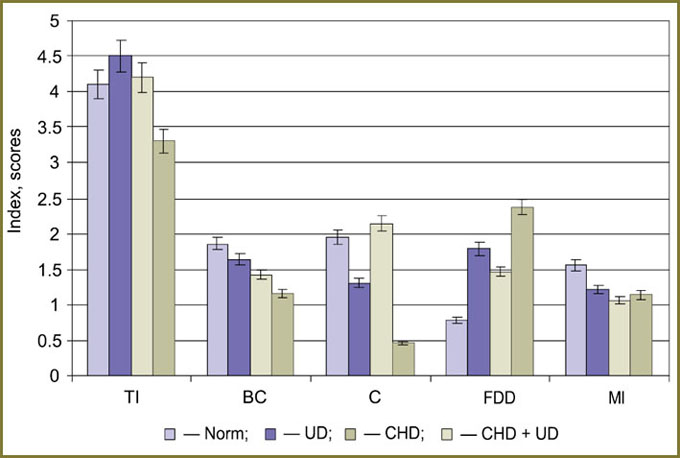 Fig. 8. Visuametry of oral fluid teziograms of apparently healthy subjects and patients with isolated and combined pathology of cardiovascular system and a middle part of GI tract. Conventional symbols are shown in Fig. 2 and 6 Fig. 8. Visuametry of oral fluid teziograms of apparently healthy subjects and patients with isolated and combined pathology of cardiovascular system and a middle part of GI tract. Conventional symbols are shown in Fig. 2 and 6
|
The signs of subtotal destruction of elements in the samples additionally suggest the intensity of pathological transformation of physicochemical properties and component composition of mixed saliva of patients with combined CHD and gastric ulcer (See Fig. 8).
Thus, it can be argued that the combined pathology has specificity in the development of crystallogenic properties of facies of biological fluids in patients with CHD and UD. This fact is consistent with dysmetabolic changes integrating the diseases under study and being due to the presence of Helicobacter pylori [1–4, 9, 10, 13, 14]. It seems obvious to distinguish several main components of CHD and UD comorbidity pathogenesis, among them: the disorders of composition and properties of proteome components of biological fluids, immune response on helicobacteriosis, etc [10, 17]. An organismic result of these metabolic changes can be myocardial malfunction (till arrhythmia development), reactions of systemic hemodynamics and microcirculation [18]. Etiological relation of these pathological conditions with Helicobacter pylori is proved by the results of numerous trials on the efficiency of eradication therapy in correction of cardiovascular disorders [19, 20, 21].
Conclusion.The study has shown that the transformation of crystallogenic activity of the properties of biological fluids in patients with isolated CHD and isolated ulcer and the combination of both, and therefore, the component composition and physic-chemical properties of biological media can appear as an indicator of the presence of metabolic response of the body on comorbidity, and also serve as a basis for the development of noninvasive techniques to monitor the efficiency of Helicobacter pylori eradication in this patient population.
Study Funding and Conflict of Interests. The study was not supported by any funds, and the authors have no conflict of interest to disclose.
References
- Aruin L.I. Helicobacter pylori: how one agent causes various diseases. Eksperimental’naya i klinicheskaya gastroenterologiya 2004; 1: 36–41.
- Bardakhch’yan E.A., et al. The role of Helicobacter pylori in the development of extragastroduodenal diseases. Eksperimental’naya i klinicheskaya gastroenterologiya 2005; 3: 20–27.
- Vasil’ev Yu.V. Acid-related gastrointestinal diseases and coronary heart disease. Lecasij vrac 2006; 1: 50–55.
- Kornienko E.A. Extragastric manifestations of Helicobacter pylori in children. Consilium medicum 2009; 1: 4–7.
- Zhang S., Guo Y., Ma Y., Teng Y. Cytotoxin-associated gene-A-seropositive virulent strains of Helicobacter pyloriand atherosclerotic diseases: a systematic review. Chin Med J (Engl) 2008; 121(10): 946–951.
- Pavlov O.N. The Helicobacter pyloricarrying as the latent system risk factor. Meditsinskiy al’manakh 2011; 4: 125–130.
- Perederiy V.G., Bezyuk N.N., Chernov A.Yu. Is there the relation between chronic infection of H. pylori and vegetative-vascular disorders in patients with functional dyspepsia. Suchasna gastroenterologіya 2004; 2: 15–18.
- Farber A.V., Zarubina I.G., Andropova O.V. Helicobacter pylori infection, atherosclerosis and coronary heart disease. Rossiyskiy kardiologicheskiy zhurnal 2003; 3: 69–71.
- Tsimmerman Ya.S. Helicobacter pylori-infection: extragastric effects and diseases (critical analysis). Klinicheskaya medicina 2006; 4: 63–67.
- Martusevich A.K., Simonova Zh.G., Tarlovskaya E.I. Helicobacter pylori and cardiovascular pathology: is really the way to the heart through the stomach? Rossijskij kardiologiceskij zurnal 2012; 3: 91–101.
- Gulyaeva S.F., Martusevich A.K., Pomaskina T.V. Mathematical modeling of induced saliva crystallogenesis results as an efficiency criterion of mineral water taking. Ekologiya cheloveka 2005; 7: 33–35.
- Martusevich A.K., Kolevatykh E.P. Crystalloscopic picture of biofluids in ulcer disease. Eksperimental’naya i klinicheskaya gastroenterologiya 2006; 6: 35–40.
- Pellicano R., Fagoonee S., Rizzetto M., Ponzetto A. Helicobacter pylori and coronary heart disease: which directions for future studies? Crit Rev Microbiol 2003; 29(4): 351–359.
- Rasmi Y., Raeisi S. Possible role of Helicobacter pylori infection via microvascular dysfunction in cardiac syndrome X. Cardiol J 2009; 16(6): 585–587.
- Kamakin N.F., Martusevich A.K. About the technique of biofluid teziocrystalloscopy. Klinicheskaya laboratornaya diagnostika 2002; 10: 3.
- Martusevich A.K., Kamakin N.F. Crystallography of biological fluid as a method of evaluating its physicochemical characteristics. Bull Exper Biol Med 2007; 143(3): 385–388.
- Kayo S., Ohsawa M., Ehara S., et al. Oxidized low-density lipoprotein levels circulating in plasma and deposited in the tissues: comparison between Helicobacter pylori-associated gastritis and acute myocardial infarction. Am Heart J 2004; 148(5): 818–825.
- Loginov S.V., Kozlova I.V., Shvarts Yu.G. Myocardial repolarization indices, heart rhythm disorders in patients with combined coronary heart disease and gastroesophageal reflux disease depending on helicobacteriosis presence and degree. Vestnik aritmologii 2005; 42: 57–60.
- Andraws R., Berger J.S., Brown D.L. Effects of antibiotic therapy on outcomes of patients with coronary artery disease. A meta-analysis of randomized controlled trials. JAMA 2005; 293(21): 2641–2647, http://dx.doi.org/10.1001/jama.293.21.2641.
- Kowalski M., Konturek P.C., Pieniazek P., et al. Prevalence of Helicobacter pylori infection in coronary artery disease and effect of its eradication on coronary lumen reduction after percutaneous coronary angioplasty. Dig Liver Dis 2001; 33(3): 222–229.
- Martusevich A.K., Vorob’ev A.V., Grishina A.A., Russkikh A.P. Crystallostasis physiology and pathology: a general paradigm and investigation prospects. Vestnik Nizhegorodskogo universiteta im. N.I. Lobachevskogo 2010; 1: 135–139.









