Compression of Great Cervical Vessels in Nodular Goiter as Indication for Thyroidectomy
The aim of the investigation was to study clinical and instrumental manifestations of the compression of carotid arteries and internal jugular veins in nodular goiter, and estimate thyroidectomy as a decompression technique.
Materials and Methods. We examined and operated on 13 patients with bilateral nodular euthyroid goiter, III–IV–V degree. The patients aged from 28 to 58 years. Thyroidectomy was indicated by the compression of trachea in 11 patients and the compression of trachea and esophagus — in 2 patients.
In addition to conventional pre- and postoperative studies the patients underwent duplex scanning of carotid arteries and internal jugular veins, fundoscopy, and contrast multidetector computed tomography (MDCT) of cervical vessels.
Results. All patients in the thyroid above nodules were found to have phlebectasia of one or both internal jugular veins with reduced linear blood flow velocity, while at the level of the nodules and beneath linear velocity increased. Three patients appeared to have common carotid arteries extended and compressed to the outside, and MDCT in one patient revealed total contrast absence of a part of the carotid artery at nodular level and no contrast of the internal jugular vein on the same side. Fundoscopy showed the presence of wide straight veins and narrow arteries. After nodular goiter resection, phlebectasia of internal jugular veins disappeared, linear blood flow velocity normalizing, and dislocated carotid arteries being straightened.
Conclusion. In addition to tracheal and esophageal compression, the compression of great cervical vessels in nodular goiter is no less important indication for thyroidectomy.
Nodular abnormalities in thyroid diseases are found by palpation in 5% subjects, while by ultrasound — almost 5–10 times more frequently [1]. In most cases these nodular masses after morphological examination using fine-needle aspiration biopsy are verified as colloid proliferative goiter, which, according to semisentenary observations, is never malignized. Thus, currently, the surgical indications in nodular goiter are the following: cosmetic defect due to cervical deformity and decompression syndrome, by which tracheal and esophageal compression is meant by.
According to a few reports in the recent years, nodular abnormalities in thyroid can also compress great vessels of the anterior cervical surface [2].
Artery compression can result in the spasm due to periarterial plexus irritation and worsened hemodynamic indices. As a result, patients complain of dizziness, increased fatigability, weakness, and hypomnesia [3].
The increase in thyroid volume only by 1.4 times is known to result in common carotid artery stenosis and jugular vein dilatation [2]. Cerebral circulation grows worse significantly due to reduced blood filling of brain vessels and decreased venous drainage. Consequently, marked vegetovascular disorders develop.
If blood outflow in internal jugular veins is impaired, venous encephalopathy develops. In long-term encephalopathy, in addition to headaches, there is a sense of “strutting” in the head with eye bulb “pushing out”, head noises, hearing impairment, blurring, vision dimout, and seeing spots [4].
The aim of the investigation was to study clinical and instrumental manifestations of the compression of carotid arteries and internal jugular veins in nodular goiter, and estimate thyroidectomy as a decompression technique.
Materials and Methods. Annually, in surgicalclinic named after A.I. Kozhevnikov, N.A. Semashko Nizhny Novgorod Regional Clinical Hospital, over 300 operations for nodular goiter with tracheal compression, less frequently — with esophageal compression, are performed. In 2014 the condition of carotid arteries and internal jugular veins in 13 patients with nodular goiter and the mentioned compression syndrome was examined. Among patients there were 1 male and 12 female. The patients’ age varied from 28 to 58 years, the duration of the diseases being from 3 to 20 years. The patients complained of the neck size gain, hoarseness, dysphonia, breathlessness and dysphagia, dizziness and tinnitus.
12 patients were found to have multinodular bilateral goiter, 1 — multinodular right goiter. 11 patients had III degree of thyroid enlargement according to Nikolaev (1955), 1 male patient — IV degree, and 1 female patient — V degree.
Thyroid volume was from 17.9 to 145.0 cm3, the norm for male being 7.7–22.6 cm3, for female — 4.55–18.00 cm3.
The study of thyroid hormones showed euthyroid state. Ultrasound-guided fine-needle aspiration biopsy enabled to confirm the presence of proliferative goiter.
Duplex scanning of cervical vessels was performed on an ultrasound scanner Philips-HD 11 XL (Holland) using a linear probe with frequency of 5–9 MHz. We determined the wall density and the diameter of carotid arteries, their permeability and linear blood flow velocity. There were also determined the permeability and sizes of internal jugular vein at different levels, and linear blood flow velocity in them.
Ophthalmological examination [5] included: visometry, ophthalmoscopy, photo recording of the tissues of the ocular fundus using a fundus-camera (Topcon, Japan), vessel calibrometry with arteriolovenular coefficient (AVC) calculation by the ratio of arteriole cross-section area to venule cross-section area. The diameter of vessels was calculated according to А.А. Tryaskov technique (1966). Normal AVC is 0.83.
Multidetector computed tomography (MDCT) of the neck was performed according to a standard program with intravenous bolus dose of Ultravist-370 for cervical vessel angiography to determine the ratio of nodular masses in thyroid to carotid arteries and jugular veins.
The study complies with the declaration of Helsinki (adopted in June, 1964 (Helsinki, Finland) and revised in October, 2000 (Edinburg, Scotland)) and approved by the Ethics Committee of Nizhny Novgorod State Medical Academy. Writteninformedconsentwasobtainedfromallpatients.
The data were statistically processed using a computer program Statistica 6.0. For comparison of three studied groups we used Friedman rank analysis of variance, to compare the samplings by a quantitative criterion — Wilcoxon test with Bonferroni correction for multiple testing. Selective parameters had the following symbols: Me — median, Q1 — higher quartile, Q3 — lower quartile, n — volume of the subgroup under study, p — the value of statistical significance of differences. Critical value of significance value was taken equal to 5% (p≤0.05).
Results and Discussion. It has been found that in III–IV–V degree nodular goiter, venous regional hemodynamics suffer more frequently due to the compression of internal jugular veins. Higher pressure in common carotid arteries and denser arterial wall make them less pressure compliant by thyroid nodes compared to internal jugular veins located nearby. In three patients with thyroid volume of 145, 140.5 and 102.9 cm3 common carotid arteries had no direct route but were displaced to the outside with a slight lumen narrowing. MDCT showed no contrast of the common carotid artery at the node level. Volumetric and linear blood flow velocity in carotid arteries did not differ significantly from the norm. Three patients were found to have atherosclerotic plaques different in size in the internal carotid arterial orifice, one female patient — the increase in intima-media layer thickness.
Jugular vein compression was found in 13 of 12 patients with nodular goiter including a patient with thyroid volume — about 20 cm3, while in another patient with thyroid volume of 74.4 cm3 no compression was revealed. The compression of both internal jugular veins was found in 6 cases, the right internal jugular vein compression — also in 6 cases. There was no isolated left compression of this vein. The sizes of the internal jugular vein above the compression appeared to be 18 [16; 18] × 12 [11; 13] mm, the norm being 15×15 mm. The average linear blood flow velocity above the compression was 19.2 [15.7; 26] cm/s, and at the compression level — 60.3 [34.7; 71] cm/s that was significantly higher (p=0.009).
On examination 2 patients were found to have the steady dilatation of the internal jugular vein of the compressed side on the right, duplex scanning confirming the finding. It indicated the impaired extracranial venous outflow in the neck. In one patient with the right internal jugular vein compression MDCT also revealed a narrow tortuous vein, contrast following in it from the right thyroid lobe to the internal jugular vein.
Ophthalmoscopy of each patient included 10–15 measurements of arterial and venous caliber after the second bifurcation of central retinal vessels, since they were the most susceptible to pathological changes. Arterial narrowing and vein dilatation were visualized in all cases. AVC in the group of 5 patients was 0.648 [0.625; 0.79] indicating retinal angiopathy.
Regional hemodynamic changes in the examined patients with nodular goiter were consistent with a subclinical (latent) stage of the pathological process, there being no marked and clear subjective manifestations of the impaired hemodynamics.
Thyroidectomy was performed to correct the compression in bilateral goiter, and hemithyroidectomy — the compression in unilateral goiter. Such volume of the operation was also due to the fact that there was no healthy tissue in the thyroid. After the operation the patients paid attention that there were no discomfort in the neck, breathlessness, dysphagia, dizziness and headache. Postoperative control duplex scanning of common carotid arteries showed their straight course, normal volumetric and linear blood flow velocity. The sizes of the internal jugular veins after compression correction decreased up to 14.5 [13; 16] (p=0.0022) and 10 [8; 10] mm (p=0.0044).
The average linear blood flow velocity in them decreased up to 25 [23.5; 26.5] cm/s (norm — 20–30 cm/s) that was significantly lower than the same index at the compression level preoperatively (p=0.014), and became equal along the whole length of the vessel. In addition, there was found the significant increase of blood flow velocity above the compression level after the compression correction (p=0.046). The decompression of the internal jugular veins resulted in the disappearance of the internal jugular vein dilatation.
The control postoperative fundoscopy showed flow-dependent dilatation of arterial vessels and the narrowing of veins. AVC increased compared to the initial value up to 0.856 [0.846; 0.86] (p=0.043) indicating the improved arterial blood supply and venous outflow from orbital structures, as well as the reduced risk of vascular complications.
Here we provide a clinical observation confirming the presence of the compression of great cervical vessels by thyroid nodes in bilateral goiter and the compression correction after thyroidectomy.
A 57-year-old female patient L. was admitted to Surgical clinic named after А.I. Kozhevnikov on March, 26, 2014. On admission she complained of enlarged and deformed neck, dysphagia, breathlessness and dizziness. She noticed the enlargement of the neck 20 years ago, but sought medical advice only in November 2013 due to dysphagia. The patient had a concomitant disease — type 2 diabetes mellitus.
The general state was satisfactory. AP — 130/90 mm Hg, pulse — 84 bpm. Respiration — vesicular, respiration rate — 18 per minute. There was revealed external respiratory impairment — of restrictive and obstructive type. The patient’s face was puffy, cyanotic. The neck was uniformly deformed due to the enlarged thyroid from one sternocleidomastoid muscle to another. Each thyroid lobe had a conglomerate of dense painless nodes, from the left the conglomerate extending behind the sternum. When swallowing, the nodes were displaced upwards, no skin adhesions. Lymphatic nodes were not enlarged.
The volume of the left lobe — 77.5 cm3, the right lobe — 67.5 cm3. According to Nikolaev (1955) degree V thyroid enlargement was diagnosed (Fig. 1, а).
 Fig. 1. A 57-year-old patient L.: а — preoperative; b — postoperative Fig. 1. A 57-year-old patient L.: а — preoperative; b — postoperative
|
Thyroid hormones: thyrotropic hormone (TTH) — 0.98 μIU/ml; free T4 — 14.1 pmol/L; antithyroperoxidase (anti-TPO) — 1.00 IU/ml. According to the cytological examination — cytogram of colloid goiter.
Duplex scanning of cervical vessels showed the following: the common carotid arteries were permeable; in the left internal carotid artery orifice there was located atherosclerotic plaque, with its lumen narrowed by 24%. The internal jugular vein to the right of the thyroid node was dilated up to 18 mm (the norm: 15×15 mm) (Fig. 2, а).
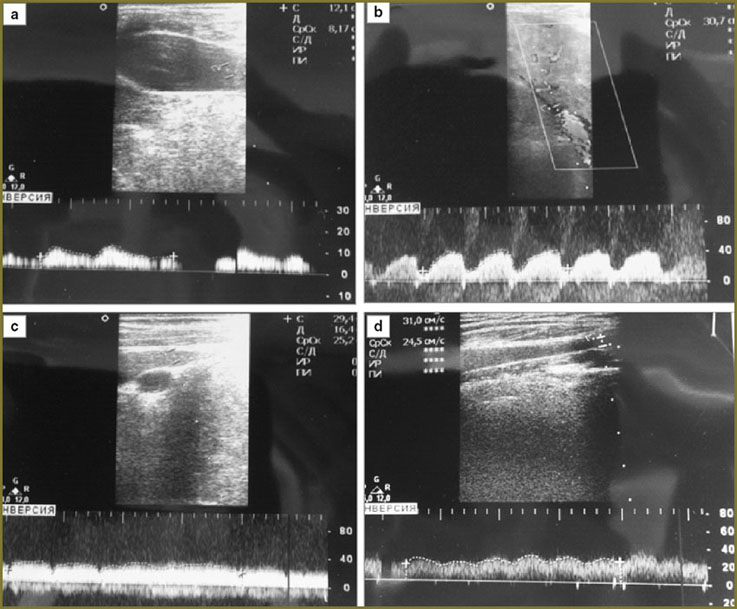
Maximum linear blood flow velocity at this level was 12.1 cm/s, the average linear velocity — 8.1 cm/s. Maximal linear blood flow velocity at the level of the node and below was 44.1 cm/s, the average linear velocity being 30.7 cm/s (Fig. 2, b).
The size of the internal jugular vein on the left above the node was 14×15 mm. Maximum linear blood flow velocity at this level was 18.1 cm/s, and the average linear velocity — 14.2 cm/s. At the level of the node and below the velocities were equal — 29.4 and 25.2 cm/s (Fig. 2, c).
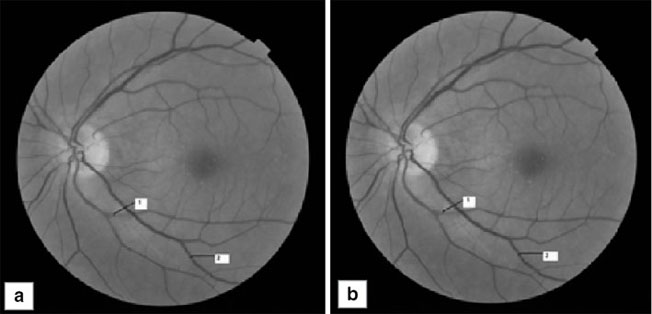
Fundoscopy showed the marked angiopathy of retinal vessels on both sides. The veins were dilated, full-blood (especially, on the right) and straightened. AVC was 0.79, the norm being 0.83 (Fig. 3, а).
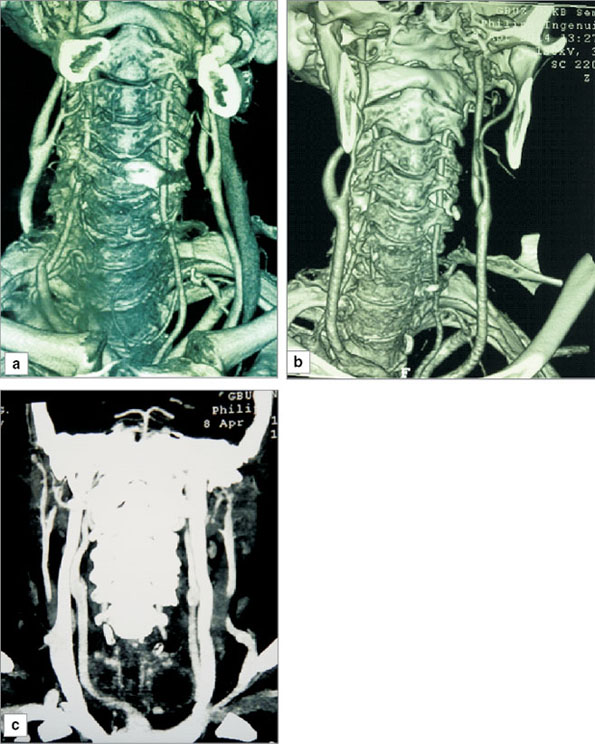
Contrast MDCT showed the thyroid nodes to prevent the straight route of common carotid arteries pushing them to the periphery and compressing (Fig. 4, а). No contrast of the internal jugular vein to the right is also due to the compression.
Thus, current diagnostic techniques enable to reveal reliably the compression of great cervical vessels in nodular goiter without specific complaints in patients with this pathology. It cannot be ruled out that the atherosclerotic plaque appeared in the left internal carotid artery orifice of the patient due to the thyroid node pressure on the common carotid artery with an impaired laminar blood flow in it.
The patient underwent thyroidectomy on April, 2, 2014. When the thyroid was surgically released, the compression of the common carotid arterial nodes on the right and the compression of internal jugular veins were found (Fig. 5).
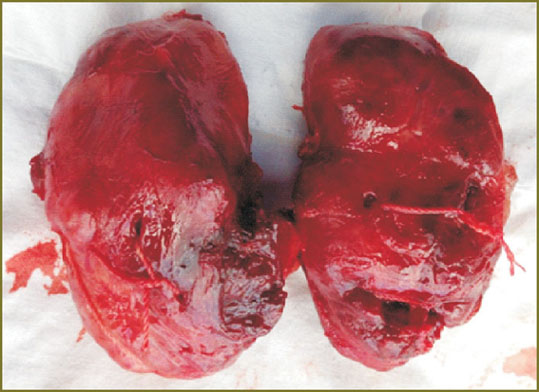 Fig. 5. The removed thyroid with nodes Fig. 5. The removed thyroid with nodes
|
The postoperative period was uneventful.
The control examination of the cervical vessels showed the following. Duplex scanning demonstrated the internal jugular vein to be permeable along its whole length, its sizes decreasing up to 16×12 mm. Maximum linear blood flow velocity in this vein along its length was 31 cm/s, the average linear velocity — 24.3 cm/s (See Fig. 2, d). The internal jugular vein to the left was permeable along its length, the vein size being 12312 mm, maximum linear blood flow velocity was 19–21 cm/s, the average linear velocity — 20.6 cm/s. Fundoscopy showed reduced full-blood and dilatation of retinal veins and their straightening. AVC grew up to 0.83 (See Fig. 3, b).
Contrast MDCT of cervical vessels enabled to reveal positive dynamics of their condition: the common carotid arteries obtained their straight course, neither local narrowing nor filling defects were found, the level and the pattern of the bifurcations of the carotid arteries were typical, the internal and external carotid arteries being symmetrical on either side (See Fig. 4, b). The internal jugular veins were clearly contrasted as well (See Fig. 4, c).
The patient was discharged for outpatient therapy under the care of an ophthalmologist and an angiosurgeon.
Conclusion. In degree III–IV–V (according to Nikolaev) nodular goiter, in addition to tracheal and esophageal compression, there is also the compression of common carotid arteries and internal jugular veins. Vascular component of the compression can have no intensive subjective and clinical manifestations, but it is fraught with the risk of vascular abnormalities of the brain. Duplex scanning of cervical vessels, multodetector computed tomography of the neck with angiography, and fundoscopy enable to detect the compression of the mentioned vessels.
Operative measures — thyroidectomy or hemithyroidectomy — offers the opportunity to correct radically the compression of common carotid arteries and internal jugular veins.
Study Funding and Conflict of Interests. The study was not supported by any financial sources, and the authors have no conflict of interest to disclose.
References
- Fadeyev V.V. Nodular goiter: controversial problems and negative tendencies in clinical practice. Klinicheskaya i eksperimental’naya tireoidologiya 2007; 3(2): 5–14.
- Mladentsev P.I., Reznichenko S.G., Mladentseva T.V. Kompleksnoe lechenie tyazhelykh form autoimmunnogo tireoidita. V kn.: Sovremennye aspekty khirurgicheskoy endokrinologii [Complex treatment of severe autoimmune thyroiditis. In: Current aspects of surgical endocrinology]. Saint Petersburg; 2003; p. 156–158.
- Ul’yanova A.E. Kliniko-funktsional’naya kharakteristika narusheniy regionarnoy gemodinamiki i ikh rannyaya diagnostika pri uzlovykh obrazovaniyakh shchitovidnoy zhelezy u zhenshchin. Dis. … kand. med. nauk [Clinical and functional characteristics of regional hemodynamic abnormalities and their early diagnosis in nodular goiter in women. Dissertation for the degree of Candidate of Medical science]. Ivanovo; 2009.
- Troshin V.D., Gustov A.V., Smirnov A.A. Sosudistye zabolevaniya nervnoy sistemy [Blood vessel diseases of nervous system]. Nizhny Novgorod: Izd-vo NGMA; 2006.
- Stepushina О.А., Bolshunov А.V., Smetankin I.G. Combined use of adaptive optics and calibrometry in retinal vein occlusion prognosis in venous occlusion of fellow eye in patients with refraction anomalies. Sovremennye tehnologii v medicine 2012; 2: 109–112.









