A Case of Cerebrocardiac Syndrome
There has been described a case of cerebrocardiac syndrome. Infarction-like ECG changes were found in a patient with subarachnoid hemorrhage in cerebral basilar artery zone with brain edema development that resulted in hyperdiagnosis of acute coronary pathology.
The term “cerebrocadiac syndrome” was suggested in the middle of 50-s of the last century to designate ECG changes, accompanying damage of the brain. In a wider sense, cerebrocardiac syndrome means the presence of a whole set of cardiac disorders in patients with acute cerebral events including various clinical and instrumental changes (ventricular arrhythmias, cardialgias, cerebrogenic pulmonary edema, infarction-like ECG changes). A principal statement is that these changes are often not the signs of the damage of the heart itself, but reflect the pathology of the brain.
Cerebrocardiac syndrome may arise in acute disturbance of cerebral circulation, craniocerebral trauma, subarchanoid and intracranial bleedings, brain tumors, encephalitis, neuroinfections, comas of different genesis. The mentioned states are frequently accompanied by the damage of the stem vegetative centers and impairments of the cardiovascular autonomic regulation with hypersympathicotonia. Extreme toxic effect of cathecholamines, in its turn, may result in metabolic damage of the myocardium with various clinical and instrumental manifestations.
The problems associated with cerebrocardiac syndrome are diagnostic errors and hyperdiagnosis of cardiac pathology in the situations when it is actually not present, and, respectively, incorrect treatment.
Patient B., aged 56, was brought by the ambulance to the reception ward of the therapeutic in-patient department with a diagnosis “acute cardiovascular insufficiency”. The woman was in sopor, did not respond to questions. It was found that she lost her consciousness in the city bus. Later her relatives said that she had been suffering from hypertension for a long time.
On admission her condition was assessed as heavy. There was no consciousness, AP was 160/120 mm Hg, HR — 100 per min. Respiration was noisy, 22 per min, moist rales were heard over all pulmonary fields, a pink foam was discharged from the mouth.
ECG revealed: sinus rhythm, negative T waves recorded in leads I and aVL, pathologic Q wave and elevation of ST segment — in leads V1–V2 (Fig. 1, a). A pathologic Q wave was also recorded in the chest leads, being one and two intercostal spaces higher (Fig. 1, b).
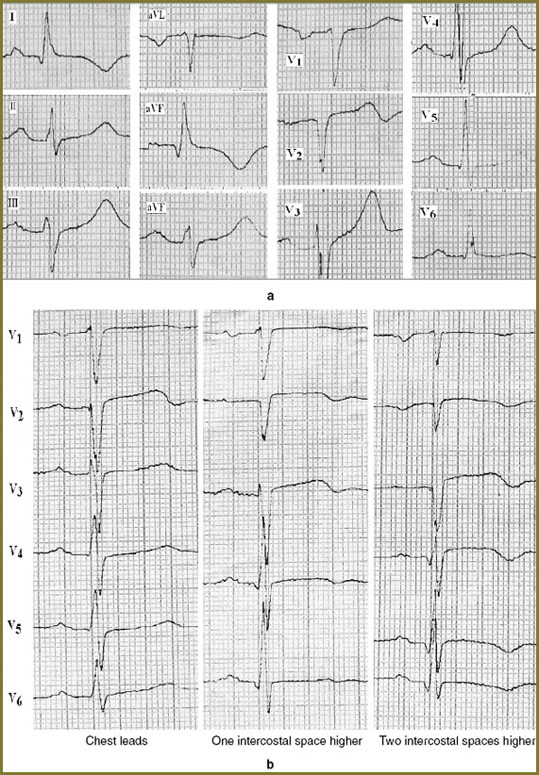 Fig. 1. ECG of the patient with cerebrocardiac syndrome: a — in standard 12 leads; b — in chest leads one or two intercostal spaces higher Fig. 1. ECG of the patient with cerebrocardiac syndrome: a — in standard 12 leads; b — in chest leads one or two intercostal spaces higher
|
According to the clinical picture (pulmonary edema, arterial hypertension) and ECG changes a doctor on duty made a diagnosis “coronary heart disease: high anterolateral Q-myocardial infarction” and hospitalized the patient to the resuscitation unit. Further dynamic observation demonstrated a certain variability of ECG (Fig. 2), which formally spoke of the changes going on in the myocardium. The analyses showed an increase of creatine kinase MB fraction (34–34–24.4 U/L; normal values up to 25 U/L), AST (54–139–190.6 U/L; normal values up to 40 U/L), LDH (662–966 U/L; normal values 207 — 414 U/L), leukocytosis — up to 18·109/L. The patient stayed in the unit for 6 days, remaining unconscious. Pulmonary edema was removed on admission, but later signs of vascular insufficiency were observed and inotropic support of myocardium was required. Hospital doctors suspected the possibility of a stroke but absence of focal neurologic symptoms did not allow them to confirm the diagnosis.
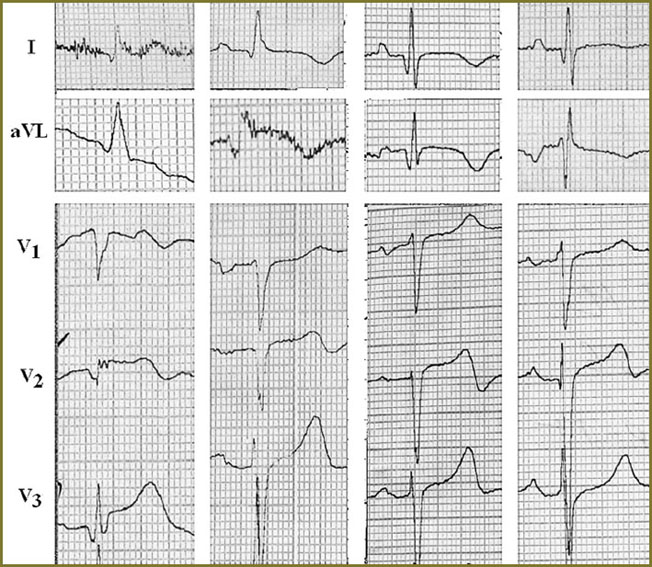 Fig. 2. ECG dynamics of the patient with cerebrocardiac syndrome Fig. 2. ECG dynamics of the patient with cerebrocardiac syndrome
|
In 6 days after progressing cardiovascular insufficiency the patient died. The autopsy findings showed that the cause of death was subarachnoid extensive hemorrhage in the zone of the cerebral basilar artery with the development of the medullary substance edema. No signs of myocardium damage were determined during autopsy. Coronary arteries turned out to be patent, their walls were thin, elastic with a smooth intima. Microscopic examination did not reveal any foci of myocardium micronecrosis.
The case described demonstrates typical manifestations of cerebrocardial syndrome, when infarction-like ECG changes were not manifestations of the heart damage (which, according to the autopsy data, appeared to be intact), but a reflection of the involvement of the stem structures of the brain in subarachnoid hemorrhage.
It should be noted, that pulmonary edema which occurred in the patient at the beginning of the disease, may not only be of cardiogenic genesis but also of the central one as well due to the damage of the respiratory center.
Study Fundingand Competing Interest. This study was not supported by any financial sources and there is no topic specific conflict of interest related to the authors of this study.









