Modern Possibilities of Kidney Ultrasound Diagnosis in Children
The aim of the investigation was to study the possibilities of complex ultrasonography (using shear wave elastography and power Doppler mapping of the intrarenal vessels) for evaluation of the renal parenchyma as a method of early non-invasive diagnosis in children suffering from obesity and metabolic syndrome.
Materials and Methods. Kidney ultrasound examination was performed using portable digital ultrasound system ANGIODIN-Sono/P-Ultra (BIOSS, Russia). Forty-two children were examined using shear wave elastography of the renal parenchyma and power Doppler mapping for evaluation of intrarenal vessels.
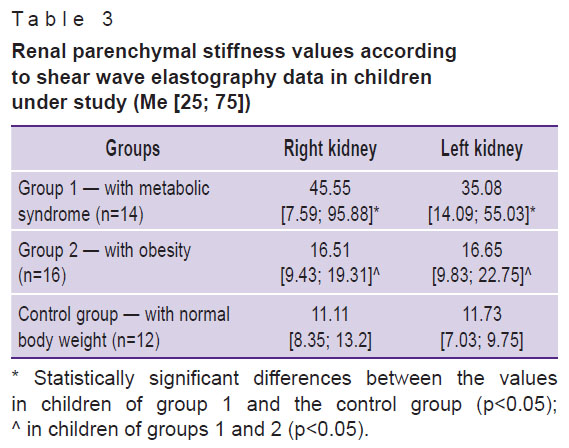
Results. Children with obesity and metabolic syndrome were found to have high frequency of registering renal blood flow types 2, 3, and 4 which characterize the decline in its intensity. According to shear wave elastography results, statistically significant differences in renal parenchymal stiffness were revealed in children with obesity and metabolic syndrome, children with metabolic syndrome and control group children (with normal body weight). Renal parenchymal stiffness value in children with obesity was likely to be higher (p>0.05) than in control group children. The revealed changes in renal parenchymal stiffness values in children with metabolic syndrome may speak of vasospasm on the capillary level (the glomeruli), which can be followed by remodeling of the glomerular wall, particularly, against the background of systemic arterial hypertension. This increases the risk of vicious cycle formation: ischemia of the renal parenchyma and activation of juxtaglomerular apparatus ↔ persistence and exacerbation of arterial hypertension. In children with obesity and metabolic syndrome, the mode of power Doppler with a standardized evaluation scheme provides the possibility to identify the intensity of renal blood flow due to high reproducibility of the technique.
Conclusion. Complex use of modern renal ultrasound techniques (shear wave elastography + power Doppler mapping) gives the possibility to reveal the group of high cardiovascular risk in children with obesity.
Obesity and overweight are closely associated with the development of metabolic syndrome whose markers are diabetes mellitus type 2, arterial hypertension (AH), early atherosclerosis, gastrointestinal tract pathology, reproductive disorders, oxidative stress [1−6]. Recent investigations show that obesity is considered to be an independent risk factor for chronic renal diseases. Insulin resistance, hyperinsulinemia and dyslipidemia found in metabolic syndrome promote AH. Hormonal-metabolic disorders and AH, in turn, affect structural-functional state of the kidneys and lead to glomerulopathy development [7, 8].
Renal tissue stiffness can be evaluated quantitatively (this value elevation evidences initiation of parenchymal changes) using a new method of ultrasound diagnosis, shear wave elastography [9]. The operating principle of this technique is based on generating shear waves inside the tissue of interest and subsequent assessment of the wave travel velocity [10]. Today, shear wave elastography technique is applied to diagnose liver, mammary gland and thyroid gland diseases [9, 11]. Only occasional studies devoted to the use of this technique for diagnosing kidney diseases suggest that shear wave travel velocity is influenced by various factors, including renal blood flow [12]. Currently, the method of color Doppler mapping and its variants called power Doppler are used to assess renal hemodynamics. In the modes of color and power Doppler mapping, the diameter of the vessels is determined, the location of intrarenal vessels and the degree of renal parenchyma vascularization are evaluated [13, 14].
Power Doppler is superior to color Doppler in visualization of normal intrarenal vasculature due to the ability to register low-velocity flows and it is used to identify areas of ischemia in the kidneys [15, 16]. A comprehensive renal ultrasound examination in B-mode, shear wave elastography and power Doppler mapping allow physicians to obtain the most objective picture characterizing structural and functional conditions of the kidneys and to diagnose renal disorders in the early stages of development.
Thus, it is challenging from scientific and practical points of view to evaluate the possibilities of modern ultrasound techniques (shear wave elastography, power Doppler mapping of intrarenal vessels) for diagnosing different kidney pathologies, especially in children.
The aim of the investigation was to study the possibilities of complex ultrasonography for evaluation of the renal parenchyma (using shear wave elastography and power Doppler mapping of the intrarenal vessels) as a method of early non-invasive diagnosis in children suffering from obesity and metabolic syndrome.
Materials and Methods. There were examined 42 patients aged 11 to 17 years who underwent inpatient treatment in Pediatric Department No.1 of Smolensk Children Clinical Hospital in 2014−2015. Anthropometric measuring included body weight (kg), height (cm), waist circumference (cm), body mass index. General clinical examination involved general blood test and urine analysis. Biochemical blood assay was performed using Hitachi 912 apparatus (Hitachi, Japan) to identify the parameters of lipid metabolism (total cholesterol, triglycerides, high-density lipoproteins (HDL), low-density lipoproteins (LDL), very low-density lipoproteins (VLDL)) and carbohydrate metabolism (glucose), fibrinogen and C-reactive protein. Renal function was assessed by Zimnitskiy’s test, glomerular filtration rate was estimated using Schwarts formula. The oral glucose tolerance test was performed on automated biochemical rapid-response analyzer Innova Star (Diasys Diagnostic System, Germany). Urinary albumin excretion was evaluated by semi-quantitative analysis using diagnostic system MicroalbuPHAN (Erba Lachema, Czech Republic). 24-hour blood pressure monitoring was carried out using BPLAB apparatus (Russia).
Obesity classification based on body mass index percentiles was used in the study with reference to age and gender of a particular person.
All patients were divided into three groups. Group 1 included 14 children and adolescents with metabolic syndrome. According to recommendations of International Diabetes Federation (IDF, 2007), inclusion criteria in the group were the presence of abdominal obesity, atherogenic dyslipidemia (hypertriglyceridemia and/or decrease in HDL cholesterol level). Group 2 comprised 16 patients with primary uncomplicated exogenous-constitutional obesity. The control group consisted of 12 children and adolescents of the second health group with normal body weight. Children of all three groups had no history of urinary tract lesions.
The study complies with the Declaration of Helsinki (adopted in June 1964, Helsinki, Finland and revised in October 2000, Edinburgh, Scotland) and was performed following approval by the local ethics committee of Smolensk State Medical University. Written informed consent was obtained from all patients aged 15–17 and the parents of those patients who were under 15 in accordance with the Federal Law “The Basic Law on the Health Protection of the citizens of the Russian Federation” dated July 22, 1993, No.487-1.
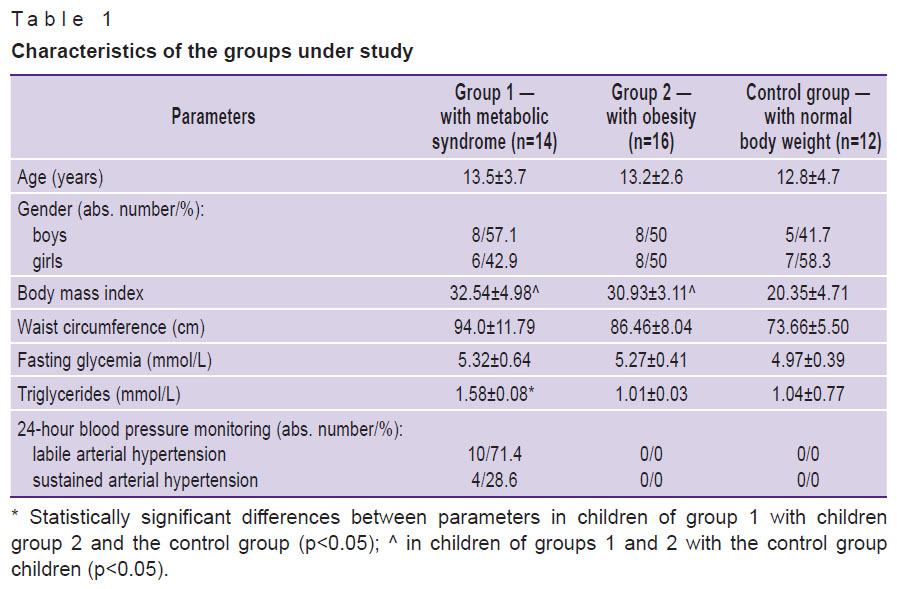
When evaluating anthropometric parameters, a tendency (p>0.05) towards higher body weight values was revealed in the group of children with metabolic syndrome compared to the children with obesity. Similar tendency was observed in relation to body mass index values (Table 1).
|
Table 1. Characteristics of the groups under study |
When estimating carbohydrate metabolism, blood glucose levels were found to be corresponding to impaired fasting glycemia in a single case. On the whole, no differences in glycemia level were found in children of groups 1 and 2. Lipid profile analysis demonstrated statistically significant increase in triglyceride levels in children with metabolic syndrome compared to the children with obesity. Mean levels of total cholesterol, HDL, LDL, atherogenic index had no statistically significant differences.
High-risk grade I AH was observed in all children with metabolic syndrome. According to 24-hour blood pressure monitoring results, labile hypertension was registered in 71.4% of children, 28.6% had sustained AH.
Kidney ultrasound examination was performed using portable digital ultrasound system ANGIODIN-Sono/P-Ultra (BIOSS, Russia) with 3–6 MHz electronic curvilinear transducer, the patient being in prone position. Anatomical assessment of the kidneys was carried out in B-mode to determine the size, location, contours of the kidneys, parenchymal cortex echogenicity.
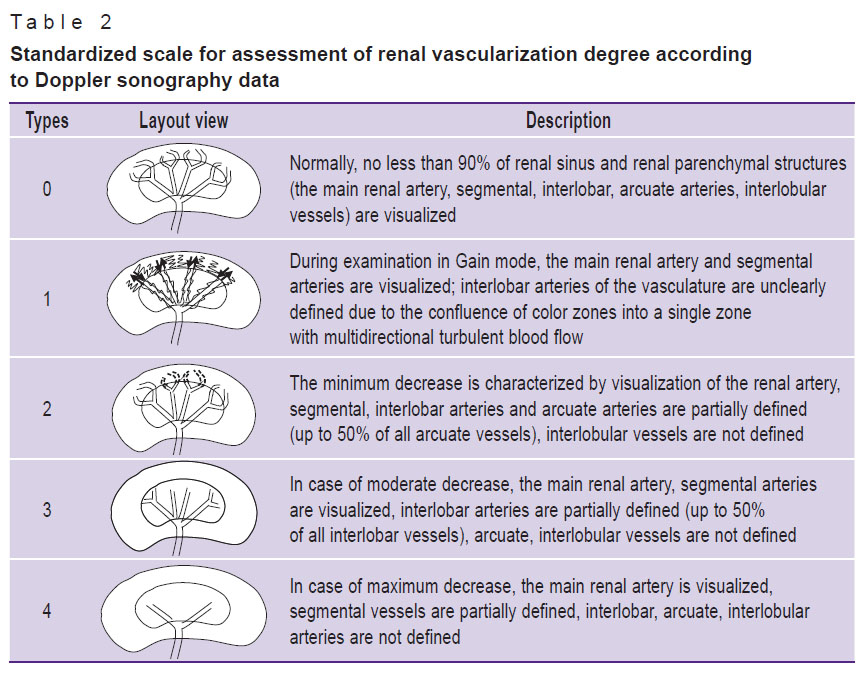
The mode of power Doppler mapping available with this device ensured high-quality assessment of renal blood flow in the longitudinal section of the kidney area. Multiplanar scanning was performed exporting the images of segmental arteries 4–5 to the assessment zone during the procedure to ensure reliability of the conducted examination. Such exporting segmental arteries 4–5 implies multiplanar scanning to visualize the blood flow during a single ultrasound examination by one specialist for 1–5 min. To evaluate vascularization degree of the renal parenchyma in adults, in 2000, Bertolotto et al. suggested a five-point scale for intrarenal blood flow assessment: preserved blood flow to the renal capsule was assigned 4 points with its gradual decrease down to 0 points when no parenchymal blood flow was detected. To assess vascularization degree of the renal parenchyma in children, a modified five-point Bertolotto scale proposed by Barsukov et al. was used in the study [17] (Table 2). According to power Doppler data, type 1 blood flow in children was characterized by blood flow increase and its decrease was classified as types 2–4.
|
Table 2. Standardized scale for assessment of renal vascularization degree according to Doppler sonography data |
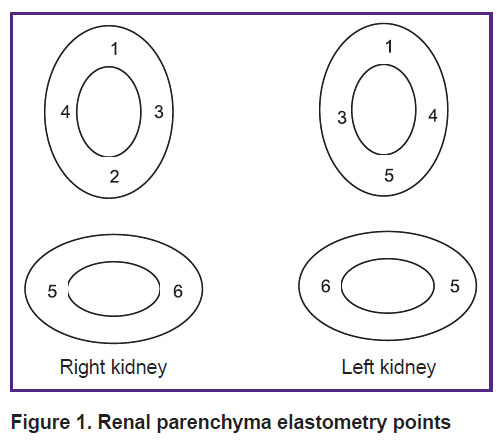
Shear wave elastography of the renal parenchyma was performed in 6 points with longitudinal and transverse scanning. The selection of points was determined by the anatomic structure of the kidney (Figure 1). Shear wave technology is quantitative elastometry providing the possibility to select the examination region. When making optimal gray-scale renal examination, in conditions of good and steady visualization, the mode of shear wave elastography was used to determine the digital stiffness value of the examined renal parenchymal volume in kilopascals (kPa). The mean stiffness value was registered when the deviation identified therewith amounted to no more than 30% of the mean value [18]. On the display, stiffness of the examined renal parenchyma region was coded on the background of the gray-scale image in the form of a color image. The renal parenchyma region characterized by high stiffness values was mapped in red color, the one with low values was displayed in blue color. On the display, stiffness values were registered in kPa.
|
Figure 1. Renal parenchyma elastometry points |
Statistical data processing was performed by means of Microsoft Excel 2000 and Statistica 7.0 software. The resulting data were presented as mean value and standard deviation (for data with normal distribution), median and interquartile interval (for data with non-normal distribution). The differences were considered statistically significant at p<0.05.
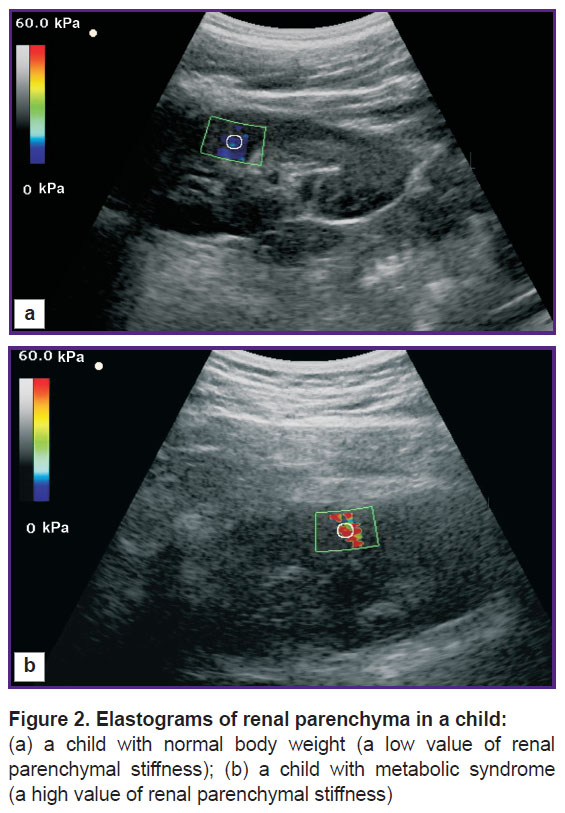
Results. Shear wave elastography data (Table 3) showed statistically significant differences in renal parenchymal stiffness in children with obesity and metabolic syndrome as well as in those with metabolic syndrome and control group children. Renal parenchymal stiffness value in children with obesity tended to increase (p>0.05) compared to control group children. Figure 2 shows ultrasound images of kidneys of a control group child and a child with metabolic syndrome.
|
Table 3. Renal parenchymal stiffness values according to shear wave elastography data in children under study (Me [25; 75]) |
|
Figure 2. Elastograms of renal parenchyma in a child: (a) a child with normal body weight (a low value of renal parenchymal stiffness); (b) a child with metabolic syndrome (a high value of renal parenchymal stiffness) |
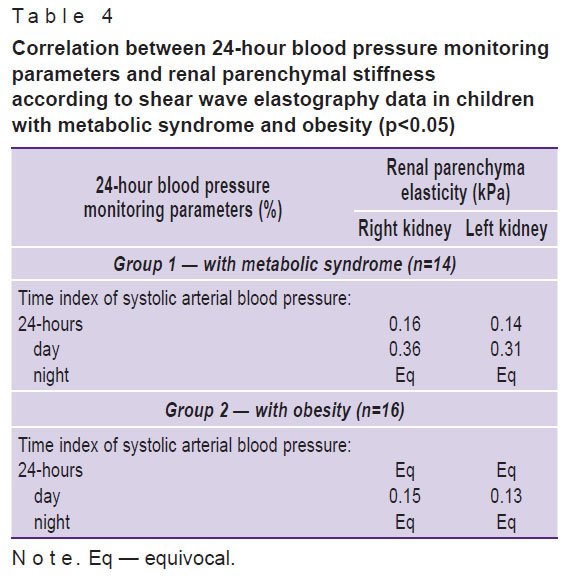
According to shear wave elastography data, correlation analysis of 24-hour blood pressure monitoring parameters, time index of systolic AP and renal parenchymal stiffness, revealed statistically significant weak direct correlation between time index of systolic AP and renal parenchymal stiffness in children with metabolic syndrome (Table 4), this correlation being very weak in children with obesity.
|
Table 4. Correlation between 24-hour blood pressure monitoring parameters and renal parenchymal stiffness according to shear wave elastography data in children with metabolic syndrome and obesity (p<0.05) |
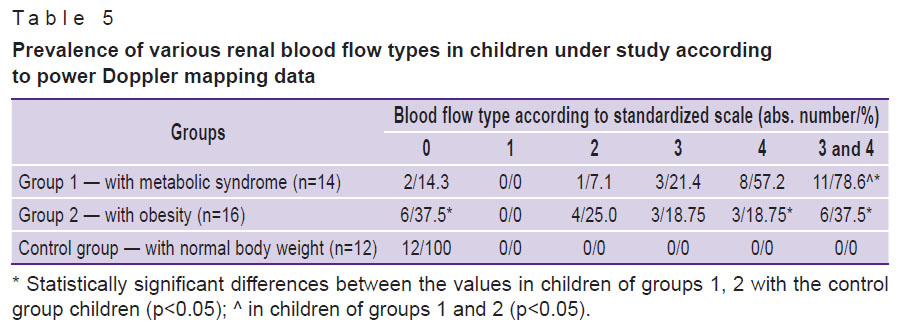
When carrying out qualitative evaluation of renal blood flow in the mode of power Doppler mapping using the standard technique, the following blood flow types were registered (Table 5): normal renal blood flow (type 0) was found in 2 children of group 1, 6 children of group 2 and in every one of 12 control group children.
|
Table 5. Prevalence of various renal blood flow types in children under study according to power Doppler mapping data |
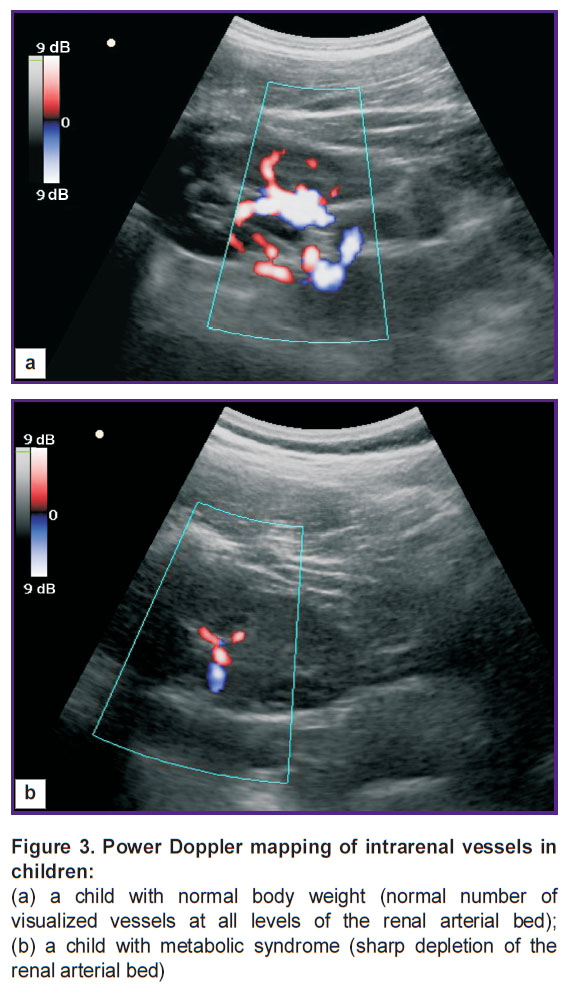
Figure 3 shows power Doppler mapping images of the intrarenal vessels in a control group child (type 0) and a child with metabolic syndrome (type 4).
|
Figure 3. Power Doppler mapping of intrarenal vessels in children: (a) a child with normal body weight (normal number of visualized vessels at all levels of the renal arterial bed); (b) a child with metabolic syndrome (sharp depletion of the renal arterial bed) |
Discussion. Evaluation of renal blood flow, an essential part of the blood circulation system, is necessary for revealing risk factors of cardiovascular complications. The role of kidneys in regulation of vascular tone and arterial pressure is significant. AH has been proved to develop in conditions of renin–angiotensin–aldosterone system hyperactivation in metabolic syndrome [7]. Human adipose tissue produces many elements of this system: angiotensin I, II, renin, angiotensinogen, types I and II angiotensin receptors, angiotensin transforming enzyme [3, 19]. Excessive production of vasoconstrictive factors is observed in obesity against the background of endothelial dysfunction. For example, angiotensin II causes the following adverse effects: vasoconstriction, aldosterone, vasopressin and noradrenaline secretion, fluid retention, smooth muscle cell proliferation, sympathoadrenal system activation. Affecting the renal structures, angiotensin II causes their hypertrophy, hyperplasia. As the number of arterial pressure elevation events and their duration increase, vascular structural changes develop, moderate medial hypertrophy is observed [20].
The revealed changes in renal parenchymal stiffness values in children with metabolic syndrome may speak of vasospasm on the capillary level (the glomeruli), which is consistent with power Doppler mapping findings evidencing intrarenal blood flow decrease. Later, this may be followed by remodeling of the renal vessel wall, particularly, against the background of systemic arterial hypertension in children with obesity. As a result, the risk of vicious cycle formation increases: ischemia of the renal parenchyma and activation of juxtaglomerular apparatus ↔ persistence and exacerbation of arterial hypertension. This statement is based on indirect methods of evaluating structural changes in the kidneys. The use of direct methods of examination such as angiography and renal biopsy is strictly limited in children and they are administered only on the grounds of life-saving indications. Therefore, noninvasive diagnostic techniques acquire particular applicability.
Conclusion. In children and adolescents with obesity and metabolic syndrome, it is appropriate to carry out complex ultrasound examination of the renal parenchyma. Overweight patients with high values of renal parenchymal stiffness proved by shear wave elastography data and intrarenal blood flow decrease revealed on power Doppler mapping should be referred to a group of high risk for metabolic syndrome marker formation, particularly, arterial hypertension. The revealed renal structural-functional changes in children and adolescents with obesity and metabolic syndrome suggest the necessity of administering metabolic therapy within a complex treatment program: endothelioprotective medications (antioxidants etc.), medications improving microcirculation (antiaggregants etc.).
Study Funding and Conflict of Interests. This study was not supported by any financial sources and the authors have no conflicts of interest to disclose.
References
- Bekezin V.V., Kozlova L.V., Kovalenko O.M., Leonov S.D., Feodorov G.N., Peresetskaya O.V. Features of free radical oxidation in children and adolescents with obesity and metabolic syndrome. Profilakticheskaya i klinicheskaya meditsina 2009; 2: 49–53.
- Bokova T.A. Etiopathogenesis of metabolic syndrome in children. Lechenie i profilaktika 2011; 1: 50–55.
- Dedov I.I., Mel’nichenko G.A., Butrova S.A. Fat tissue as an endocrine organ. Ozhirenie i metabolizm 2006; 1: 6–13.
- Pavlovskaya E.V., Kaganov B.S., Strokova T.V. Obesity in children and adolescents: pathogenic mechanisms, clinical manifestations, treatment approaches. Mezhdunarodnyy zhurnal pediatrii, akusherstva i ginekologii 2013; 3(2): 67–79.
- Peterkova V.A., Vasyukova O.V. About the new classification of obesity in the children and adolescents. Problemy endokrinologii 2015; 61(2): 39–44.
- Shilov A.M., Avshalumov A.Sh., Sinitsina E.N., Eremina I.V. Risk factor correction in overweight patients with insulin resistance and arterial hypertension. Russkiy meditsinskiy zhurnal 2011; 19(13): 805–811.
- Ivashkin V.T., Drapkina O.M., Korneeva O.N. Klinicheskie varianty metabolicheskogo sindroma [Clinical variants of metabolic syndrome]. Moscow: Izdatel’stvo “Meditsinskoe informatsionnoe agentstvo”; 2012; 216 p.
- Palm F., Nordquist L. Renal oxidative stress, oxygenation, and hypertension. Am J Physiol Regul Integr Comp Physiol 2011; 301(5): R1229–R1241, https://doi.org/10.1152/ajpregu.00720.2010.
- Zykin B.I., Postnova N.A., Medvedev M.E. Elastography: method anatomy. Promeneva diagnostika, promeneva terapiya 2012; 2–3: 107–113.
- Rudenko O.V., Safonov D.V., Rykhtik P.I., Gurbatov S.N., Romanov S.V. Physical bases of elastography. Part 2. Shear wave elastography (lecture). Radiologiya — praktika 2014; 4: 62–71.
- Borsukov A.V., Kryukovskiy S.B., Pokusaeva V.N., Nikiforovskaya E.N., Peregudov I.V., Morozova T.G. Elastografiya v klinicheskoy gepatologii (chastnye voprosy) [Elastography in clinical hepatology (specific issues)]. Smolensk: Smolenskaya gorodskaya tipografiya; 2011; 276 p.
- Bob F., Bota S.,
Sporea I.,Sirli R.,Petrica L., Schiller A. Kidney shear wave speed values in subjects with and without renal pathology and inter-operator reproducibility of acoustic radiation force impulse elastography (ARFI) — preliminary results. PLoS One 2014; 9(11): e113761, https://doi.org/10.1371/journal.pone.0113761. - Glazun L.O., Polukhina E.V. Ul’trazvukovaya diagnostika zabolevaniy pochek [Ultrasound diagnosis of kidney diseases]. Moscow: Vidar; 2014; 296 p.
- Poleshuk L.A. The characteristic of renal blood flow at children with kidney diseases (review). Nefrologiya i dializ 2006; 8(3): 225–231.
- Bude R.O., Rubin J.M., Adler R.S. Power versus conventional color Doppler sonography: comparison in the depiction of normal intrarenal vasculature. Radiology 1994; 192(3): 777–780, https://doi.org/10.1148/radiology.192.3.8058946.
- Babcock D.S., Patriquin H., LaFortune M., Dauzat M. Power Doppler sonography: basic principles and clinical applications in children. Pediatr Radiol 1996; 26(2): 109–115, https://doi.org/10.1007/bf01372087.
- Borsukov A.V., Bekezin V.V., Kozlova E.U. Standardization of quality evaluation of Doppler ultrasonography of the kidneys in children with obesity and metabolic syndrome. Vestnik Smolenskoy gosudarstvennoy meditsinskoy akademii 2015; 14(2): 34–37.
- Dynnik O.B., Linskaya A.V., Kobylyak N.N. Shear wave elastography and liver parenchyma elastometry (methodological issues). Promeneva diagnostika, promeneva terapiya 2014; 1–2: 73–82.
- Shestakova M.V. Activity of the adipose tissue angiotensin-renin system (RAS): metabolic effects of RAS blockage. Ozhirenie i metabolizm 2011; 1: 21–25.
- Nazarenko G.I., Khitrova A.N., Krasnova T.V. Sovremennye meditsinskie tekhnologii i dopplerograficheskie issledovaniya v uronefrologii [Modern medical technologies and Doppler sonography in uronephrology]. Moscow: Meditsina; 2002; 152 p.








