A Case of Transcranial Duplex Scanning of Cerebral Arteries in a Patient with Neurotrauma
There has been described a clinical case to demonstrate the capabilities of transcranial duplex scanning (TCDS) in brain death diagnosis. The feature of the technique is the detection of brain circulation stagnation staging: from alternating circulation to a total absence of Doppler spectrum in all intra- and extracranial arteries of brachiocephalic system including all standard imaging approaches, among them transorbital imaging of intracranial vessels. The identification of alternating circulation in extracranial vessels enables to verify stagnation of brain circulation regardless intracranial blood flow indices that is of great importance in case of bad quality of bone window for TCDS.
The necessity of using additional diagnostic tests when there are difficulties in assessing clinical condition of CNS is supported by the majority of researchers [1–4]. Ultrasound techniques occupy the leading position among all noninvasive examination modalities due to their informativity, reproducibility, safeness for the patient, the possibility of conducting bedside dynamic observations [5, 6]. In modern devices duplex scanning of intracranial vessels enables to make quantitative assessment of blood flow in a pulse-wave mode, in the mode of color mapping, and in the B-mode, simultaneously. In the investigations of the Russian and foreign authors a high comparability of transcranial duplex scanning data with the findings of cerebral angiography has been shown [1–4, 7].
Below, a clinical case from our practice is presented.
Patient D., born in 1984, fell down and hurt his head as a result of a generalized epilepsy. With a heavy cerebrocranial trauma he was delivered to the Central District Hospital. On admission he was conscious and complained of a headache. Computed tomography (CT) of the brain revealed intracerebral hematomas of the frontal areas from both sides, epidural hematoma of the left parietal area, fracture of the skull base. During three hours from the admission the level of his consciousness dropped to sopor. An emergency surgery was performed — resectional craniotomy, removal and external drainage of the epidural hematoma (100 ml in volume). Patient’s post-operative condition was assessed as extremely heavy, the level of consciousness — I–II grade coma. On the 3rd day dynamic CT-examination showed multiple hematomas of the right brain hemisphere, intracranial hematoma of the left parietotemporal area.
On the 5th day from the injury the patient was transferred to the department of neuroresuscitation and intensive care of one of the hospitals of Nizhny Novgorod. On admission the suppression of consciousness was noted to be II grade coma (according to the Glasgow coma scale (GCS) — 4–5 scores), AP — 110/65 mm Hg, HR — 82 per min. Magneto-resonance imaging (MRI) revealed multiple intracerebral hematomas of the cerebral hemispheres with perifocal edema; in the brain stem there was a zone of the altered signal 40×35×50 mm (the majority of data speak in favor of hematoma); ventricle IV was not visualized; compression of the cerebellum vermis was observed; the right lateral ventricle and ventricle III of the brain were pressed, median structures were shifted to the left by 9 mm; signs of subarachnoidaland subdural hemorrhage in the right frontotemporal area (aneurism is suspected) were also found.
According to the emergency indications (a suspected rupture of aneurism in the right hemisphere) an operation was performed — external decompression of the right hemisphere in the front-parietal-occipital area, removal of intracerebral hematomas and foci of crushing of the temporal and frontal lobe on the left, elimination of the remained epidural hematoma. Intraoperation transmural duplex scanning of the brain vessels was made, signs of cerebral angiospasm of the right medial cerebral artery with the increased velocity of the linear blood flow up to 180 cm/s were revealed.
In spite of the treatment conducted a post-operative condition of the patient remained extremely heavy. Signs of consciousness suppression to III grade coma (GCS — 3–5 scores), meningeal symptoms, absence of movement activity remained in the neurological status. In 12 h after the operation and during the following 3 days duplex scanning of intracranial vessels showed a marked diffuse angiospasm on both sides with a peak blood flow velocity in the median cerebral artery up to 220 cm/s.
On the 4th post-operative day III grade coma, atony, areflexia were observed in the neurological status. Duplex scanning of intracranial vessels did not identify the blood flow in the posterior cerebral artery on both sides, and in the anterior and median arteries of both sides in segment M1 blood flow with a high peripheral resistance and velocity 120 cm/s was revealed. Dynamically made MRI of the brain found signs of generalized edema of the brain, decrease of ventricle sizes, disappearance of differences between the gray and white substances.
On the 6th day clinical manifestations of the brain death appeared: III grade coma; atony; areflexia; moderately widened pupils (4 mm in diameter); centrally fixed; photoreaction; absence of corneal reflex; no reflex from trachea. Conducting triplex scanning, presence of bidirectional spectrum of the flows in the area of median, anterior and main arteries was noted in the projection of all visualized intracranial vessels, which reflected the signs of cerebral circulation arrest (Fig. 1).
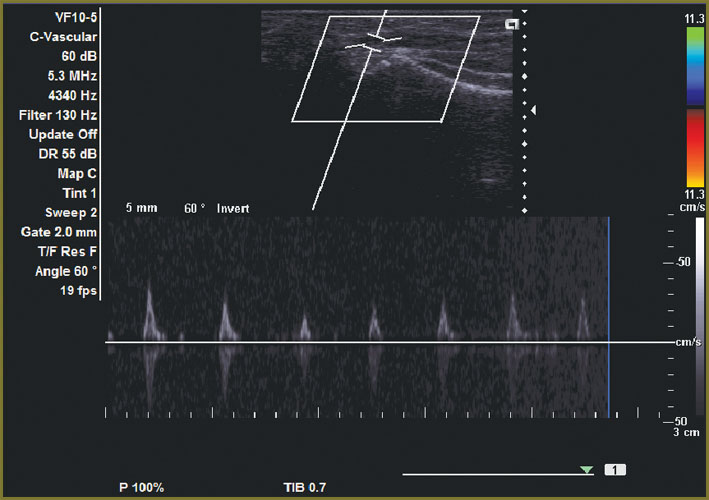 Fig. 1. DTCS, transtemporal access, right-side visualization at the level of the midbrain: bidirectional blood flow in the segment M1 of the right median brain artery Fig. 1. DTCS, transtemporal access, right-side visualization at the level of the midbrain: bidirectional blood flow in the segment M1 of the right median brain artery
|
On the next day DTCS revealed the following changes: the blood flow was not determined in the posterior brain artery on both sides, in the anterior artery it was on both sides with single loci of systolic peaks up to 50 cm/s, in the median artery in segment M1 the blood flow was noted to have a bidirectional spectrum with the velocity of 120 cm/s, in segment M2 the blood flow was in the form of systolic peaks up to 20–30 cm/s (Fig. 2).
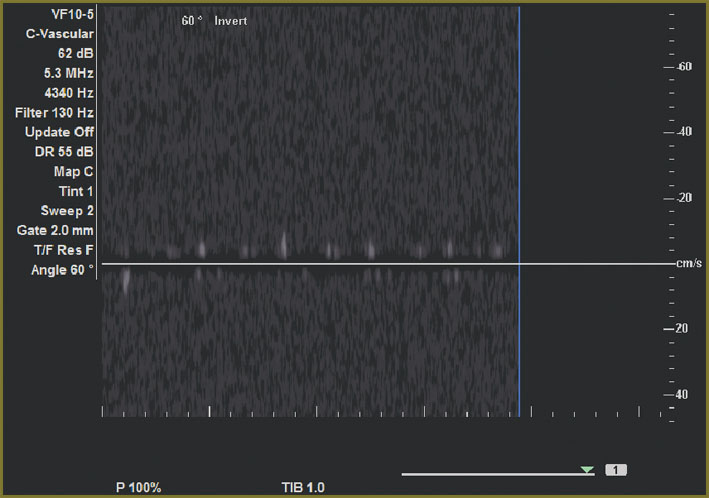 Fig. 2. DTCS, transtemporal access, right-side visualization at the level of the midbrain: unidirectional systolic blood flow in the segment M1 of the right median brain artery with less than 50 cm/s velocity Fig. 2. DTCS, transtemporal access, right-side visualization at the level of the midbrain: unidirectional systolic blood flow in the segment M1 of the right median brain artery with less than 50 cm/s velocity
|
On the 8th day from the last operative intervention and on the 14th day from the injury the patient died. Post mortem examination showed signs of generalized edema and dislocation of the brain, thrombosis of venous sinuses, necrotic changes in the stem part of the brain, initial manifestations of encephalitis.
In the clinical case described there was revealed a tendency to the decrease of velocity parameters with the increase of peripheral resistance values in the projection of all the vessels in the course of duplex scanning with the analysis of hemodynamics in the projection of extra- and intracranial arteries.
In case of brain circulation arrest indices of DTCS are usually characterized by pathognomic changes of the velocity spectrum of the main artery flows, which correspond to the perfusion cessation in the brain.
The following are the signs of intracranial blood flow arrest found by DTCS [2, 5]:
1) at the stage of alternating blood flow the sum of indices of anterograde and retrograde flow approximates to zero, which, to a great degree, correlates with the signs of circulation cessation in the brain found by color Doppler scanning, and shows fluctuations of a small amount of blood in the vessel lumen backward and forward without any advance along the bloodstream;
2) at the stage of systolic waves phases of isolated systolic blood flow are determined, the duration of which is less than 200 ms, and peak systolic velocity amounts to less than 50 cm/s without a diastolic component;
3) complete absence of Doppler spectrum.
The given clinical case clearly shows a parallel between clinical and dopplerographic signs of a heavy brain injury, resulted in its death.
According to the recommendations of Neurosonology Research Group of the World Federation of Neurology studying brain death, the diagnosis of “circulation arrest in the brain” can be established in case of the presence of the following conditions [5, 7]:
1) a combined analysis of hemodynamics in extra- and intracranial vessels supplying the brain is performed;
2) flow spectra, corresponding to circulation arrest in the brain during 30 min, are determined in the vessels;
3) insonation of all major vessels performing circulation in the brain is made — a typical picture must be detected in the projection of minimum 2 vessels, in which circulation in the brain occurs, and flow spectra are absent in other arteries;
4) visualization of the suggested diagnosis must be made by means of ultrasound scanning of extracranial segments in the common and internal carotid arteries, and vertebral arteries [3].
The clinical case described proves successful application of DTCS in the diagnosis of brain death. However, in the course of revealing brain circulation arrest incorrect verification of the findings obtained is possible due to the difficulties of visualization of intracranial vessels during application of DTCS:
1) a bad quality of insonation window, leading to the absence of flow spectra in the intracranial vessels;
2) preservation of blood flow in the intracranial vessels despite the availability of clinical and electroencephalographic signs of death, may lead to false-negative interpretation of the investigation results, as presence of persisting blood flow in the intracranial vessels, as well as electroencephalographic activity may last for some hours after the establishment of the clinical diagnosis “ brain death” [1–3].
A specific feature of this observation was the determination of the staging of circulation arrest in the brain from the appearance of alternating circulation to the complete absence of the Doppler spectrum in all intra- and extracranial arteries of brachiocephalic system, using all standard visualization approaches, including transorbital method of intracranial vessel visualization. Doppler spectra corresponding to circulation arrest in the brain were detected during 3 h.
Performing electroencephalography, bioelectrical potentials corresponding to stage I of blood flow termination registered by DTCS, were recorded. When DTCS and electroencephalography were repeated in 30 min during 3 h after the initial examination, absence of blood flow was diagnosed by the data of both examinations, which together with the clinical findings allowed to verify the brain circulation arrest.
In the course of the present observation all ultrasound methods of duplex scanning of extra- and intracranial arteries of brachiocephalic system were used. Identification of alternating character of the blood flow in extracranial vessels allows verification of brain circulation arrest independently of the indices of intracranial flow, which is of great importance when the quality of the bone window for DTCS is not good.
References
- Stulin I.D., Mnushkin A.O., Musin R.S., et al. Modern noninvasive diagnosis of brain death. Vestnik prakticheskoy nevrologii 1995; 1: 86.
- Stulin I.D. Diagnostika smerti mozga [Brain death diagnosis]. Moscow: GEOTAR-Media; 2010.
- Ducrocq X., Hassler W., Moritake K., et al. Consensus opinion on diagnosis of cerebral circulatory arrest using Doppler-sonography: Task Force Group on cerebral death of the Neurosonology Research Group of the World Federation of Neurology. J Neurol Sci 1998; 159(2): 145–150, http://dx.doi.org/10.1016/S0022-510X(98)00158-0.
- Eggers J., Pade O., Rogge A., Schreiber S.J., Valdueza J.M. TCCS successfully visualizes all intracranial parts of the internal carotid artery. Cerebrovasc Dis 2007; 23 (Suppl 1): 36.
- Val’dueza Kh.M., Shrayber S.Y., Rel’ Y-E., Klingebel’ R.K. Neyrosonologiya i neyrovizualizatsiya pri insul’te [Neurosonology and neuroimaging in stroke]. Moscow: Medpress-inform; 2012.
- Dörfler P., Puls I., Schliesser M., Mäurer M., Becker G. Measurement of cerebral blood flow volume by extracranial sonography. J Cerebral Blood Metab 2000; 20(2): 269–271, http://dx.doi.org/10.1097/00004647-200002000-00007.
- Doepp E., Schreiber S.J., Brunecker P., Valdueza J.M. Ultrasound assessment of global cerebral blood volume in healthy adults. J Cereb Blood FloorMetab 2003; 23(8): 972–977, http://dx.doi.org/10.1097/01.WCB.0000071884.63724.69.








