Cardiac Biomarkers in Patients with Isolated and Combined Course of Chronic Obstructive Pulmonary Disease and Chronic Heart Failure
The aim of the study was to define cardiac biomarkers in patients with isolated and combined chronic obstructive pulmonary disease (COPD) and chronic heart failure (CHF), to assess their level and diagnostic value in order to optimize the tactics of managing these patients.
Materials and Methods. The study included 184 patients aged 38–85 years who were divided into 3 comparison groups: group 1 (n=68) was composed of patients with I–III stage COPD (GOLD, 2017); group 2 (n=64) patients with I–III functional class CHF; group 3 (n=52) patients with a combined course of COPD and CHF. Specific cardiac biomarkers were evaluated in 80 patients (in group 1 in 26, in group 2 in 27, and in group 3 in 27 patients). Patients’ blood serum obtained by centrifuging was used for cardiac biomarker investigations.
Results. NT-proBNP (F=0.59; p=0.0490) was found to be the most sensitive biomarker for determining the severity degree of
A direct correlation has been established between the level of cardiac biomarker NT-proBNP and CHF functional class both in the isolated and combined course of COPD and CHF.
In patients highly adherent to therapy,
The levels of biomarkers have been established at which a high risk of COPD progressing to one step or higher and/or CHF to one functional class and higher is noted in comorbid COPD and CHF course.
Conclusion. The obtained data about the diagnostic value of cardiac biomarkers in
Introduction
Investigations of chronic obstructive pulmonary disease (COPD) in recent decades have been of extreme significance worldwide due to the overall prevalence, late diagnosis, large expenditures for treatment, early disability, and premature death [1, 2]. No less important is the study of chronic heart failure (CHF) which, according to the world epidemiological assessments, is one of the most widely spread, progressing, and prognostically unfavorable conditions of the blood circulation system [3, 4]. Extrapulmonary manifestations of COPD, including systemic inflammation and cardiovascular disorders allow it to be considered as a multimorbid state [5]. The main concomitant pathology essentially worsening COPD prognosis is a group of cardiovascular diseases among which ischemic heart disease (IHD), chronic heart failure (CHF), cardiac fibrillation, and arterial hypertension are distinguished [6, 7].
Difficulties of CHF diagnosis in patients with COPD, the choice of tactics and therapy methods in recent years determine an excessive scientific interest to the study of the cardio-respiratory continuum [8, 9]. The comorbidity rate, according to various data, makes from 25 to 42% aggravating significantly the outcome of the disease [10–13].
CHF and COPD are found to run intercurrently in every 3–4 cases aggravating mutually the clinical picture, worsening treatment outcomes, and increasing 2–3 times the risk of fatal cardiovascular events [12]. CHF and COPD syntropy are caused by the common risk factors (smoking, obesity, hypodynamia, etc.), similarity of some clinical signs (dyspnea, tachycardia, peripheral edemas, etc.), and community of some pathogenetic links (systemic inflammation, oxidative stress, and endothelial dysfunction).
Systemic inflammation development associated with the release of proinflammatory cytokines and oxidants into the bloodstream which induce hyperproduction of some other mediators, the level of which in various biological media may serve as a diagnostic marker at the stages of diagnosis making, choosing the tactics of comorbid patient management, assessment of dynamics, prognosis, and efficacy of the therapy conducted. The most studied markers today are CRP, IL-6, IL-8, and FNO-α [14, 15]. A number of investigations are devoted to the diagnostic value of natriuretic peptide NT-proBNP in patients with COPD [8, 16–18]. Further prospective studies are necessary to reveal and validate other clinically important markers.
Presently, many aspects of comorbid course of CHF and COPD are insufficiently studied, there are no unified algorithms of clinical decision-making based on multimarker diagnostic strategies and adequate combinations of the up-to-date pharmaceutical drugs. A more careful study of the cardio-respiratory continuum will enable the development of an optimal strategy of managing this category of patients, reduction of the rate of hospitalizations, disability, mortality, and economical losses associated with them.
The aim of the study was to define cardiac biomarkers in patients with isolated and combined course of chronic obstructive pulmonary disease (COPD) and chronic heart failure (CHF), to assess their level and diagnostic value in order to optimize the tactics of managing these patients.
Material and Methods
Prospective nonrandomized study has been carried out at City Clinical Hospital No.5 and City Clinical Hospital No.38 of Nizhny Novgorod.
The study included 184 patients aged 38–85 years who were divided into 3 groups: group 1 was composed of 68 patients (36 women and 32 men) with I–III stage COPD (GOLD, 2017), mean age 67.8 [66.24; 69.37] years; group 2 included 64 patients (43 women and 21 men) with I–III FC CHF, mean age 73.2 [71.60; 74.83] years; group 3 consisted of 52 patients (26 women and 26 men) with a combined course of I–III stage COPD and I–III FC CHF, mean age 71.2 [69.38; 72.96] years.
The study complied with the Declaration of Helsinki (2013) and approved by the Ethics Committee of Privolzhsky Research Medical University. Written informed consent was obtained from every patient.
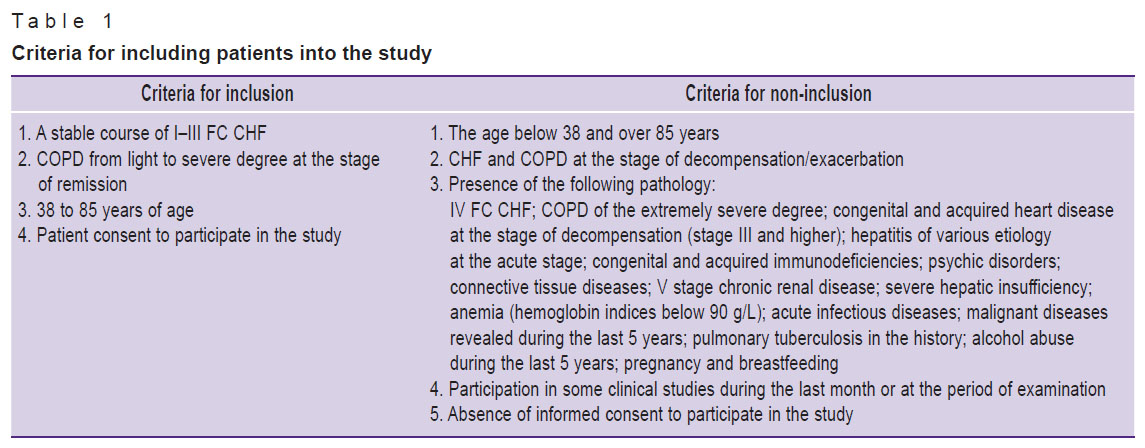
To make the results objective, criteria for inclusion and non-inclusion of patients in the clinical observation group were defined (Table 1).
|
Table 1. Criteria for including patients into the study |
After a thorough history-taking, all patients underwent a standard physical examination; assessment of anthropometric indices (height, body mass); calculation of body mass index; calculation of smoking index; the 6-minute walk test to determine the functional class of CHF (AP, HR, respiratory rate, pulse oximetry with determination of perfusion index were controlled before and after the test); echocardiography; assessment of external respiration function indices; chest radiography if indicated.
All patients included into the study were questioned in order to evaluate their general condition and quality of life using CAT (the COPD Assessment Test), CCQ (Clinical COPD Questionnaire), MLHFQ (the Minnesota Living with Heart Failure Questionnaire) and CSAS (Clinical State Assessment Scale) [19, 20]. Charlson comorbidity index was calculated for all patients. To evaluate medication adherence, Moriscos–Green scale (4-item Medication Adherence Report Scale, MARS) which has been validated and recommended for a wide application was used [21].
Two known cardiac biomarkers ST2 (interleukin-1 receptor-like protein 1 — IL1RL1) and NT-proBNP (N-terminal fragment of B-type natriuretic peptide) were chosen for determination of possible biomarkers and assessment of their diagnostic value in patients with isolated and combined COPD and CHF course.
ST2 is a protein-biomarker of cardiac stress encoded by IL1RL1 gene. It is generated in the heart in response to the pathologic changes caused by chronic diseases and/or other acute injuries, reflecting the process of ventricle remodeling and cardiofibrosis. ST2 is a predictor of CHF development while it is still in its asymptomatic phase.
NT-proBNP allows objective diagnosis of myocardium function with a high analytical sensitivity and specificity. This marker is excreted from the heart ventricles in response to their volume increase and pressure overload being therefore a marker for revealing left ventricular dysfunction. The rise of NT-proBNP concentration is connected with the increase of atria work/volume and pressure in the pulmonary artery, decrease of systolic and diastolic functions, left ventricular hypertrophy and myocardial infarction. The NT-proBNP level helps to reveal CHF at early stages and to monitor therapy efficacy.
NT-proBNP and ST2 biomarkers were evaluated in 80 patients of 184 (in group 1 in 26, in group 2 in 27, and in group 3 in 27 patients).
The biomarkers were examined using patients’ blood serum obtained by centrifuging. Fasting blood specimens were collected according to the standard procedures strictly in the morning. The results were registered using a spectrophotometer for enzyme immunoassay (EIA) (Bio-Rad, France/USA). The calibrating curves were built with the help of the software and instructions supplied with this equipment and kits. The kits from Cloud-Clone Corp. (China) designed for quantitative determination of the markers in the patient’s blood serum by the IEA sandwich-method were used in our work. Indices were determined in the range of 39–2500 pg/ml (minimal determined concentration 15 pg/ml) for NT-proBNP and 62.5–4000.0 pg/ml (minimal determined concentration 22.3 pg/ml) for ST2.
All patients received treatment in compliance with the standards of the Ministry of Health of the Russian Federation. They were dynamically followed up for a year. The following end points were fixed during the study: stable disease course, COPD progression to the next severity stage or higher and/or CHF progression to the next functional class and higher, patient death.
The statistical analysis was performed using Statgraphics plus software. Parametrical variables were compared by means of Student’s t-test for normally distributed data and Mann–Whitney test for the data which do not follow normal distribution. Bivarial variable associations were evaluated using Pearson correlation coefficients. The variables were expressed as Me [Q1; Q4] where Me is a median, [Q1; Q4] is an upper border of the first and the lower border of the fourth quartile. The qualitative data were summarized by calculating the proportion of observations (in percentage terms) of the concrete category in the examined sample. The results were considered significant at p≤0.05.
Results and Discussion
Charlson comorbidity index in group 1 was 3.8 points, in group 2 — 4.5 points, in group 3 — 5.0 points (F=2.16; р=0.1348). The data obtained during the study show that the combined COPD and CHF course differs from their isolated course by a greater severity of the pulmonary and cardiovascular system damage.
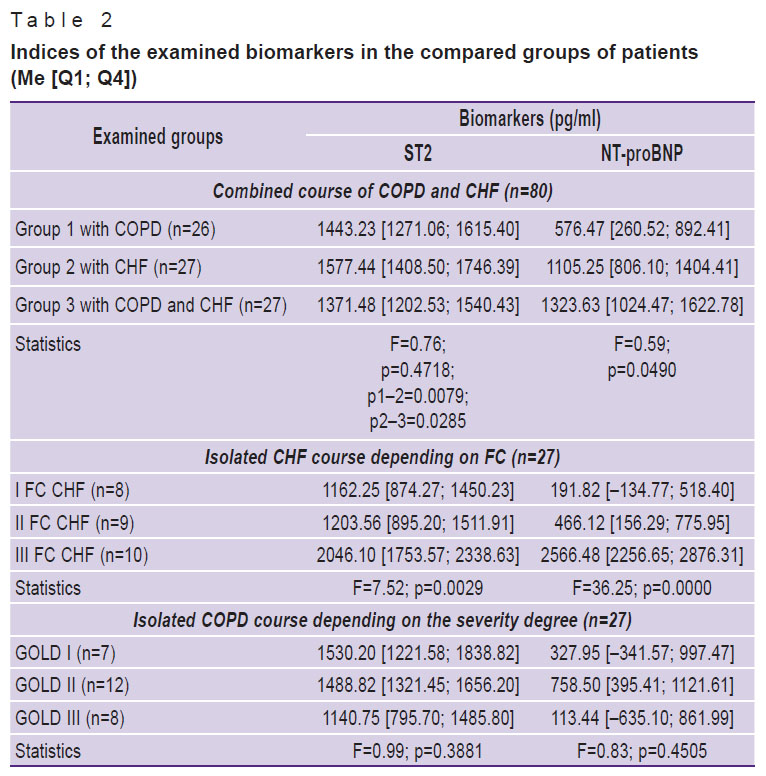
The selected marker levels have been comparatively assessed in patients with the isolated and combined course of COPD and CHF (Table 2).
|
Table 2. Indices of the examined biomarkers in the compared groups of patients (Me [Q1; Q4]) |
The comparison of ST2 level in various groups revealed its significantly higher value in people with CHF relative to the patients with COPD (p=0.0079) and with a combined COPD and CHF (р=0.0285). It speaks of a high sensitivity of ST2 biomarker in patients with cardiovascular diseases. However, this marker seems to be less sensitive in case of the combined COPD and CHF course which is confirmed by a statistically significant difference in the ST2 level in patients of group 2 and 3 (see Table 2) taking into account the fact that these groups had the same functional class of CHF.
In this connection, ST2 indices were analyzed in patients with CHF depending on FC. It is established that as FC increases, statistically significant growth of ST2 is noted in CHF patients (F=7.52; p=0.0029). The correlation between ST2 level and FC CHF was found in the isolated CHF course (R=0.342; р=0.0490) and comorbid course of COPD and CHF (R=0.307; р=0.045).
Thus, the ST2 marker reflects successfully the severity of the isolated CHF course but its diagnostic value is lower in the combined COPD and CHF course.
In COPD patients ST2 indices did not have significant differences depending on the severity degree (see Table 2).
The assessment of NT-proBNP marker discovered the tendency to its level increase in the group of patients with the combined COPD and CHF course in comparison with other groups (F=0.59; p=0.0490). It leads to the conclusion that this biomarker does not lose its sensitivity in case of the combined COPD and CHF course.
In patients with CHF, a statistically significant growth of NT-proBNP level depending on the disease FC was established (F=36.25; p=0.0000). The data obtained are confirmed by the presence of a high correlation dependence between the NT-proBNP level and FC CHF in case of the isolated course of CHF (R=0.717; р=0.0000) and comorbid course of COPD and CHF (R=0.669; р=0.0000); and also between the NT-proBNP and FC CHF in comorbid course of COPD and CHF (R=–0.542; р=0.0000).
Thus, the cardiac NT-proBNP marker reliably reflects the degree of cardiac damage severity in the isolated and combined COPD and CHF course.
In patients with COPD, a significant difference of the NT-proBNP level from the disease severity degree was not found. However, the NT-proBNP indices exceeding the values in healthy people were noted in this group which may be caused by the increase of pressure in the pulmonary artery and the development of myocardium dysfunction in presence of COPD. Therefore, on the one hand, NT-proBNP is likely to be a predictor of heart injury development still at the asymptomatic stage of the disease, on the other hand, the dependence of this biomarker on concurrent diseases should not be ignored. In this connection, the assessment of the NT-proBNP level requires taking into consideration accompanying diseases and availability of other risk factors which may raise the level of this biomarker. Unambiguous interpretation of the increased NT-proBNP level as the manifestation of CHF may lead to diagnostic errors.
Thus, among the examined cardiac biomarkers ST2 and NT-proBNP, the latter, NT-proBNP, which enables the diagnosis of heart damage at the asymptomatic stage is the most sensitive in the definition of the severity of heart damage in the combined COPD and CHF course.
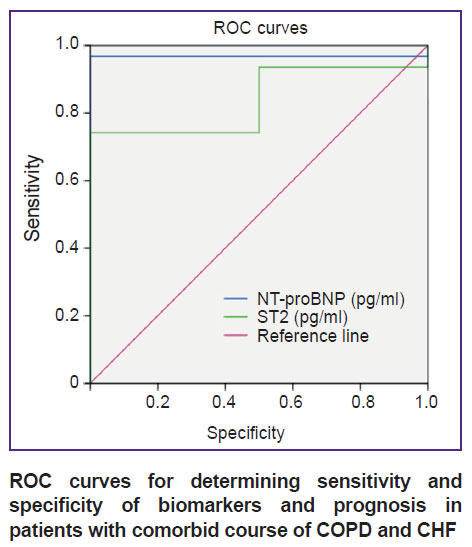
The specificity and sensitivity of biomarkers have been analyzed using ROC curves to predict the comorbid course of COPD and CHF.
The interconnection of the biomarkers with the end points in the group of patients with COPD and CHF is presented in the Figure.
|
ROC curves for determining sensitivity and specificity of biomarkers and prognosis in patients with |
According to the calculated data, a high risk of CHF progression to one FC and higher is defined in patients with the comorbid course of COPD and CHF at the level of ST2 cardiac biomarker exceeding 830 pg/ml (the area under the curve — 0.839, sensitivity — 0.871, specificity — 0.500).
At the level of NT-proBNP more than 460 pg/ml, a high risk of CHF progression to one FC and higher is defined in patients with the comorbid course of COPD and CHF (the area under the curve — 0.968, sensitivity — 0.839, specificity — 0.000).
A year-long dynamic follow-up of the patients participating in the study allowed us to determine the character of the diseases course and to analyze the end points (Table 3).

|
Table 3. |
A more stable course of COPD compared with the isolated course of CHF is noted while a more aggressive course of the diseases is observed in the group of patients with the comorbid pathology.
The relation between the disease course and patients’ medication adherence has been also investigated (Table 4).

|
Table 4. |
According to the obtained data, the disease progression was observed significantly more often in patients not adherent to medications. A negative correlation dependence was found between the medication adherence and the end points (R=–0.64985; p=0.0000).
The dependence of biomarker levels on the medication adherence is well illustrated by Table 5.

|
Table 5. Biomarker levels depending on patient therapy adherence (n=80) (Me [Q1; Q4]) |
In patients with a high medication adherence, a significant decrease of ST2 and NT-proBNP indices is noted allowing the physicians to use these biomarkers for the control of non-adherence to medical administrations.
The end point dependence on the biomarker levels has been analyzed as well (Table 6).

|
Table 6. |
A significant elevation of ST2 and NT-proBNP indices was noted in the progression of the diseases.
The data obtained show that there are no significant differences between the main groups of patients in regard to medication adherence. Less than 70% of patients demonstrated the adherence to the administered therapy regardless of the isolated or combined course of the diseases which reflects patients’ insufficient understanding of their role in maintaining their health and also speaks of the inexpediency of educational programs for patients. In the combined course of the diseases, the responsibility for their own health grows and part of the people with low adherence to therapy joins the category of high medication adherence. Moreover, the portion of non-adherent patients in all three groups appears to be almost equal and approximates to 30%.
We have also analyzed patient survival in the compared groups depending on the medication adherence using Kaplan–Meier statistical analysis. In patients with the isolated COPD course, the “fall” of the survival plot begins with the seventh month of follow-up. Prognostic survival of medication-non-adherent patients is 70% by the twelfth month of follow-up, in those with insufficient adherence 80%, and in highly adherent patients it is about 90% (χ2=22.658; р=0.000).
In patients with the isolated CHF course, the “fall” of the survival plot begins with the fifth month of follow-up. Prognostic survival of medication-non-adherent patients is 50% by the twelfth month of follow-up, in those with insufficient adherence 70%, and in highly adherent patients it is about 90% (χ2=24.800; р=0.000).
In patients with the combined COPD and CHF course, the “fall” of the survival plot begins with the fifth month of follow-up. Prognostic survival of medication-non-adherent patients is 30% by the twelfth month of follow-up, in those with insufficient adherence 40%, and in highly adherent patients it is about 70% (χ2=14.444; р=0.001).
Conclusion
The NT-proBNP (F=0.59; p=0.0490) was found to be the most sensitive biomarker for determining the degree of heart damage severity in the combined course of COPD and CHF. The ST2 biomarker reliably reflects the severity of the isolated CHF (F=0.76; p=0.0285), while in the combined course of COPD and CHF, the value of this marker decreases (F=0.76; p=0.4718).
A direct correlation has been established between the level of cardiac biomarker NT-proBNP and FC CHF both in the isolated and combined course of COPD and CHF.
In patients highly adherent to therapy, statistically significant reduction in the values of ST2 (F=3.22; p=0.0453) and NT-proBNP (F=12.20; p=0.0000) is observed which enables the physicians to control patients’ adherence to the administered therapy.
There have been established the levels of biomarkers at which a high risk of COPD progression to the next stage or higher and/or CHF to one FC and higher is noted in the comorbid COPD and CHF course.
The obtained data on the diagnostic value of cardiac biomarkers in the comorbid course of COPD and CHF is reasonable to use for therapy optimization in order to improve the quality of patient’s life and decrease the risk of unfavorable outcomes.
Study funding. The work was not supported by any financial source.
Conflicts of interest. The authors declare no conflicts of interest related to this study.
References
- Global strategy for the diagnosis, management and prevention of COPD. Global initiative for chronic obstructive lung disease (GOLD) 2017. URL: https://goldcopd.org.
- Vizel’ A.A., Vizel’ I.Yu. Chronic obstructive pulmonary disease: status of the problem in 2016. Lechashchiy vrach 2016; 4: 78–85.
- Society of Specialists in Heart Failure. Russian Society of Cardiology. Klinicheskie rekomendatsii. Khronicheskaya serdechnaya nedostatochnost’ (KhSN) [Clinical guidelines. Chronic heart failure (CHF)]. 2016 revision.
- Ponikowski P., Voors A.A., Anker S.D., Bueno H., Cleland J.G.F., Coats A.J.S., Falk V., González-Juanatey J.R., Harjola V.P., Jankowska E.A., Jessup M., Linde C., Nihoyannopoulos P., Parissis J.T., Pieske B., Riley J.P., Rosano G.M.C., Ruilope L.M., Ruschitzka F., Rutten F.H., van der Meer P.; ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37(27): 2129–2200, https://doi.org/10.1093/eurheartj/ehw128.
- Patel A.R., Hurst J.R. Extrapulmonary comorbidities in chronic obstructive pulmonary disease: state of the art. Expert Rev Respir Med 2011; 5(5): 647–662, https://doi.org/10.1586/ers.11.62.
- Davidovskaya E.I. Comorbidity in chronic obstructive pulmonary disease. Meditsinskaya panorama 2009; 9: 75–77.
- Correia L.L., Lebedev T.Y., Efremova O.A., Proshchaev K.I., Litovchenko E.S. The problem of polymorbidity in cases of chronic obstructive pulmonary disease associated with some cardiovascular diseases. Nauchnye vedomosti Belgorodskogo gosudarstvennogo universiteta. Seriya: Meditsina. Farmatsiya 2013; 4(147): 12–17.
- Gubkina V.A., Trofimov V.I., Tsvetkova L.N., Pogoda T.E., Mumortsev Y.I., Suntsov D.A. Chronic obstructive pulmonary disease and chronic heart failure in elderly people. Uchenye zapiski SPbGMU im. akad. I.P. Pavlova 2016; 23(2): 11–15.
- Kawut S.M. COPD: cardiopulmonary disease? European Respiratory Journal 2013; 41(6): 1241–1243, https://doi.org/10.1183/09031936.00009413.
- Aryal S., Diaz-Guzman E., Mannino D.M. Epidemiology of comorbidities in chronic obstructive pulmonary disease: clusters, phenotypes and outcomes. Italian Journal of Medicine 2012; 6(4): 276–284, https://doi.org/10.1016/j.itjm.2012.02.006.
- Vatutin N.T., Smirnova A.S. Treatment of comorbid chronic obstructive pulmonary disease and cardiovascular disease. Pul’monologiya 2016; 26(3): 364–371.
- Hawkins N.M., Petrie M.C., Jhund P.S., Chalmers G.W., Dunn F.G., McMurray J.J. Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology. Eur J Heart Fail 2009; 11(2): 130–139, https://doi.org/10.1093/eurjhf/hfn013.
- Kang Y., Steele B.G., Burr R.L., Dougherty C.M. Mortality in advanced chronic obstructive pulmonary disease and heart failure following cardiopulmonary rehabilitation. Biol Res Nurs 2018; 20(4): 429–439, https://doi.org/10.1177/1099800418772346.
- Chen Y.R., Chen V., Hollander Z., Leipsic J.A., Hague C.J., DeMarco M.L., FitzGerald J.M., McManus B.M., Ng R.T., Sin D.D. C-reactive protein and N-terminal prohormone brain natriuretic peptide as biomarkers in acute exacerbations of COPD leading to hospitalizations. PLoS One 2017; 12(3): e0174063, https://doi.org/10.1371/journal.pone.0174063.
- Leshchenko I.V., Baranova I.I. Biomarkers of inflammation in chronic obstructive pulmonary disease. Pul’monologiya 2012; 2: 108–117.
- Hawkins N.M., Khosla A., Virani S.A., McMurray J.J., FitzGerald J.M. B-type natriuretic peptides in chronic obstructive pulmonary disease: a systematic review. BMC Pulm Med 2017; 17(1): 11, https://doi.org/10.1186/s12890-016-0345-7.
- Nazemiyeh M., Sharifi A., Amiran F., Pourafkari L., Taban Sadeghi M., Namdar H., Abbasnezhad M. Relationship between prohormone brain natriuretic peptide (NT-proBNP) level and severity of pulmonary dysfunction in patients with chronic congestive heart failure. J Cardiovasc Thorac Res 2015; 7(1): 24–27, https://doi.org/10.15171/jcvtr.2015.05.
- Pavasini R., Tavazzi G., Biscaglia S., Guerra F., Pecoraro A., Zaraket F., Gallo F., Spitaleri G., Contoli M., Ferrari R., Campo G. Amino terminal pro brain natriuretic peptide predicts all-cause mortality in patients with chronic obstructive pulmonary disease: systematic review and meta-analysis. Chron Respir Dis 2017; 14(2): 117–126, https://doi.org/10.1177/1479972316674393.
- Khaletskaya A.I., Kuznetsov A.N., Shcherbinina E.V., Fomin I.V. Peculiarities of comorbid course of chronic obstructive pulmonary disease and chronic cardiac insufficiency and their influence on patients’ life quality. Medicinskij al’manah 2017; 3(48): 206–210.
- Khaletskaya A.I., Kuznetsov A.N. Assessment of life quality in the comorbid patients: chronic obstructive lung disease and chronic cardiac disease. Zdorov’e i obrazovanie v XXI veke 2017; 19(10): 98–101.
- Morisky D.E., Green L.W., Levine D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care 1986; 24; 67–74, https://doi.org/10.1097/00005650-198601000-00007.









{kind=link}
{kind=link}
{kind=link}